Pneumonectomy
Presentation
A 62-year-old Vietnam War veteran presents to the emergency department with complaints of acute shortness of breath. Over several months, he has had a productive cough, occasionally blood streaked, and left-sided pleuritic chest pain. He reports a decrease in his exercise tolerance as well as a 15-pound weight loss. He has a 36-pack-per-year history of smoking and drinks two or three cans of beer daily. On physical examination, vital signs are stable, temperature is 98.8°F, and oxygen saturation is 91%. Breath sounds are diminished in the left lower chest. The rest of the examination is unremarkable. In the emergency department, the following chest x-ray is obtained.
▪ Chest X-ray
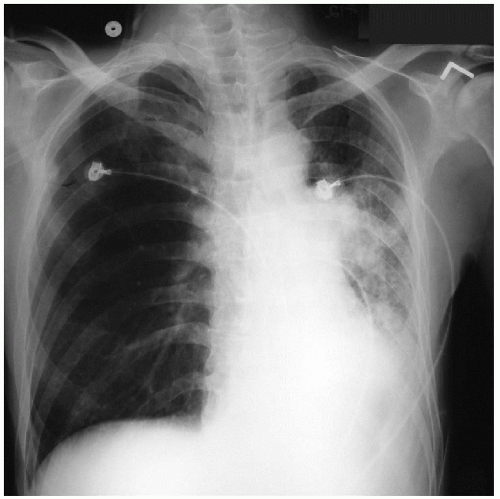 Figure 33-1 |
Chest X-ray Report
There is loss of volume of the left lung with compensatory shift of the mediastinum toward the left. The left hilum is enlarged, and there is an infiltrate at the left lung base. The right lung is hyperinflated. A fracture is present in the axillary portion of the third rib in the right chest. ▪
Case Continued
The patient was admitted for antibiotic treatment, nutritional support, and further clinical assessment. During the hospital course, the patient was more dyspneic and hypoxic (saturation 83% on room air) requiring supplemental oxygen. The following chest x-ray was obtained on the second hospital day.
▪ Chest X-ray
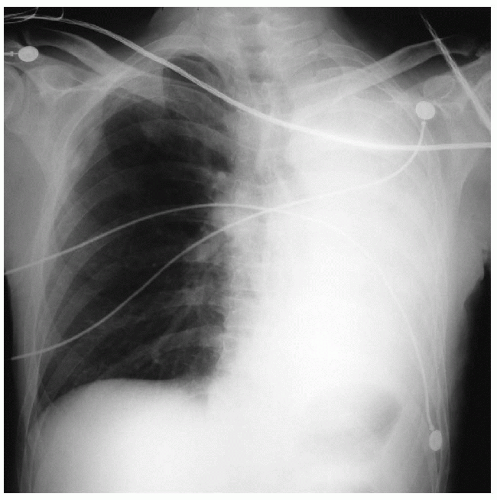 Figure 33-2 |
Chest X-ray Report
There is now total opacification of the left lung. This finding is compatible with atelectasis of the left lung, with a mediastinal shift to the left. The right lung is hyperinflated but clear of infiltrates. ▪
Recommendation
A bronchoscopy to evaluate for endobronchial lesions as well as to obtain a tissue sample for diagnosis. In addition, computed tomography (CT) scans may identify an endobronchial lesion and other disease processes that may cause bronchial obstruction.
▪ CT Scans
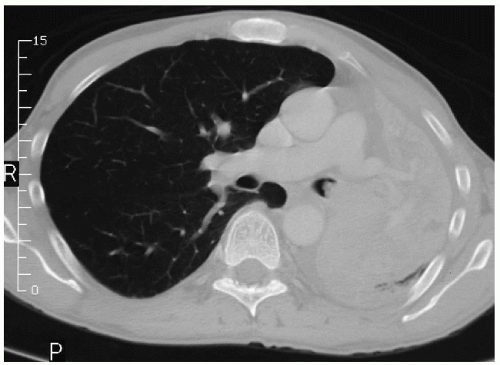 Figure 33-3 |
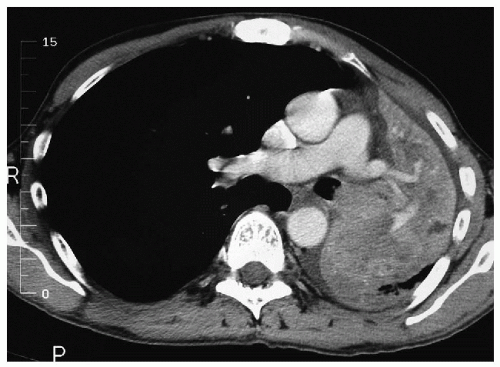 Figure 33-4 |
CT Scan Report
Most of the left lung is atelectatic, which is consistent with obstructive pneumonitis. An endobronchial mass obstructing the distal left main-stem bronchus is demonstrated. There is no mediastinal adenopathy. There is a small left pleural effusion. The right hilum and lung are unremarkable. ▪
Differential Diagnosis
Bronchogenic carcinoma is highly considered in a smoker with blood-streaked sputum and an endobronchial lesion. Other possibilities include small cell carcinoma and bronchial carcinoid with parenchymal involvement. Obstructive pneumonitis is an indicator of advanced disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


