Pneumatocele
Presentation
A 14-year-old girl is admitted to the hospital with complaints of a productive cough, fever of 102.3°F, and shortness of breath. The patient has a history of multiple episodes of pneumonia and skin infections due to a diagnosis of Job’s syndrome.
Discussion
Job’s syndrome, or hyperimmunoglobulin E syndrome, is a disease of abnormal neutrophil and monocyte chemotaxis function manifesting with recurrent infections. Patients experience multiple skin abscesses and recurrent pneumonias. Most infections are caused by Staphylococcus aureus and Candida species. Pulmonary manifestations can be associated with bronchopleural fistulas and cyst formation. Patients may also have coarse facies, restrictive lung disease, eczematous dermatitis, and scoliosis. The syndrome is inherited by autosomal dominance with variable penetrance.
Case Continued
The patient is admitted to the hospital and started on intravenous antibiotics and oxygen. A chest x-ray is obtained.
▪ Chest X-ray
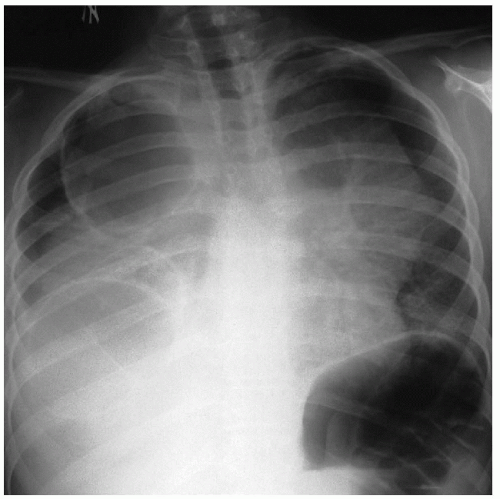 Figure 49-1 |
Chest X-ray Report
The chest x-ray demonstrates a large cystic mass occupying the upper mediastinum and both pleural spaces. The right costophrenic angle is obscured. A large gastric bubble is demonstrated in the left upper quadrant. ▪
Discussion
Pneumatoceles are thin-walled cavities most often caused by S. aureus. Pneumatoceles develop as sequelae of bacterial pneumonias in children. Although less than 3% of bacterial pneumonias in children result in formation of a pneumatocele, more than 80% of S. aureus pneumonias result in pneumatocele in the same population. Other organisms associated with pneumatocele formation include Streptococcus pneumoniae, Haemophilus influenzae, Klebsiella pneumoniae, Serratia marcescens, Escherichia coli, group A streptococci, Mycobacterium tuberculosis, and Pseudomonas aeruginosa. Pneumatoceles rapidly develop in areas of previous consolidation. Because of the rapid growth and thin walls, these cavities can rupture into the pleural space, causing a tension pyopneumothorax. In such cases, insertion of a tube thoracostomy can be life saving. Most children present with symptoms typical of pneumonia, such as fever, cough, and dyspnea. The differential diagnosis for children presenting with these symptoms includes bacterial pneumonia, pneumatocele, pulmonary sequestration, cystic adenomatoid malformation, and bronchogenic cyst.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


