Pleural Fibroma
Presentation
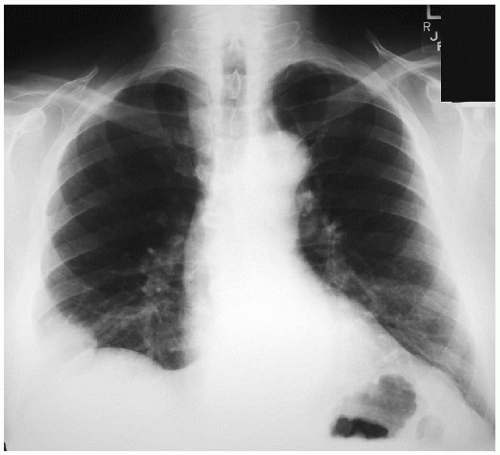
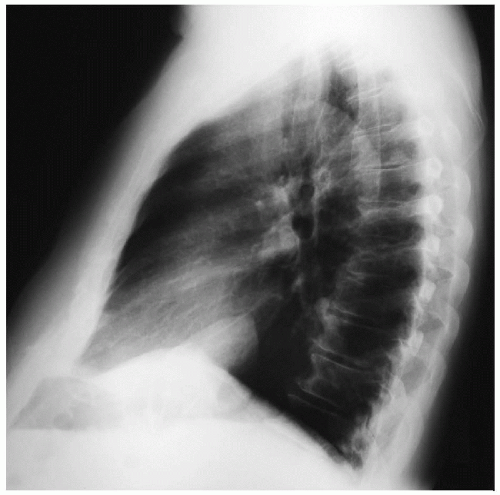
A 78-year-old woman is referred to your office by a primary medical physician with complaints of cough and right shoulder discomfort for the past 8 weeks. Additionally, she relates a history of joint pain and swelling, which has progressively worsened during the past year. The pain is a dull ache and is found in all of her joints. It is worse in her fingers and toes, and she has noticed her nail beds becoming progressively deformed during the same period of time. Her past medical history is significant for two syncopal episodes during the past year, which were found to be hypoglycemic episodes. She denies any history of smoking. There is no history of work-related or environmental exposures. On examination, the lungs are clear, the heart sounds are normal, and there are no murmurs. On examination of the extremities, there is evidence of clubbing of the fingers and toes. She presents with the following chest x-rays.
Recommendation
Computed tomography (CT) scans of the chest.
▪ CT Scans
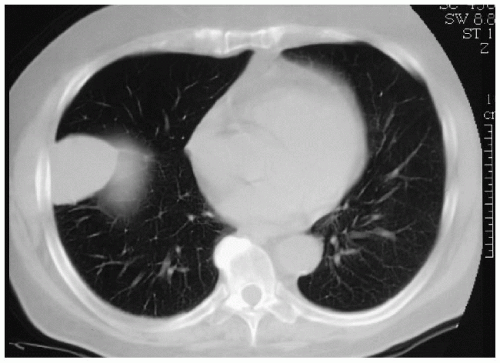 Figure 47-3 |
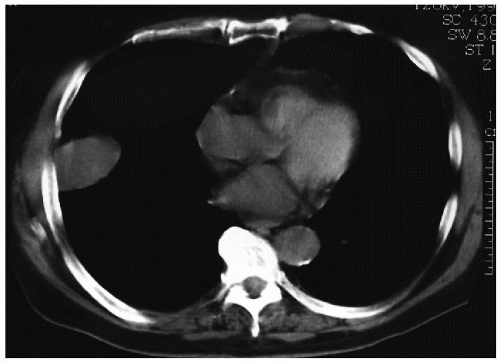 Figure 47-4 |
CT Scan Report
A smooth, oblong mass is identified in the lateral portion of the right lower lung field. The mass is homogenous and measures 5.4 cm × 4.2 cm in diameter. No other pleural or pulmonary masses are seen. The remaining lung fields are without infiltrate or effusions. The heart and aorta have appropriate opacification without aneurysmal disease. There is no evidence of mediastinal lymphadenopathy. ▪
Differential Diagnosis
The differential diagnosis of this mass includes lung cancer, metastatic tumor, and tumor of pleural origin. The smooth, rounded appearance of the lesion presents a higher likelihood of a benign, slow-growing neoplasm. Metastatic disease may be associated with prior history of a primary neoplasm. The radiologic appearance of a lung cancer is varied and remains a diagnostic possibility. Pleural fibromas are
smooth-walled, homogenous masses that can originate from the visceral or, less likely, the parietal pleura. Half of these tumors are pedunculated, enabling them to assume a dependent position. Decubitus x-rays in various positions can identify the tumor’s positional changes.
smooth-walled, homogenous masses that can originate from the visceral or, less likely, the parietal pleura. Half of these tumors are pedunculated, enabling them to assume a dependent position. Decubitus x-rays in various positions can identify the tumor’s positional changes.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


