Pharmacogenomics in Lung Cancer: Predictive Biomarkers for Chemotherapy
Pharmacogenomics in Lung Cancer: Predictive Biomarkers for Chemotherapy
Oliver Gautschi
Philip C. Mack
David R. Gandara
Rafael Rosell
Commonly used platinum-based chemotherapy regimens have shown comparable activity in randomized studies of advanced stage non-small cell lung cancer (NSCLC) patients.1,2,3 In a similar fashion, both platinum/etoposide and platinum/irinotecan are highly active in the frontline treatment of small cell lung cancer (SCLC).4,5 However, outcomes vary greatly among individual patients with the same histology, ranging from a best response of complete remission (CR) to that of progressive disease (PD). Despite the introduction of new chemotherapy drugs and molecular targeted agents in recent years, therapeutic outcomes in lung cancer patients remain poor; thus, there is a critical need for development of predictive factors to optimize selection of chemotherapy regimens for both NSCLC and SCLC and in advanced and early stages. Equally important, predictive molecular biomarkers of efficacy and toxicity could also reduce chemotherapyrelated toxicity by eliminating those patients least likely to benefit, as well as those predicted to have unacceptable levels of toxicity.
Although clinical prognostic factors for lung cancer are well established, they do not provide the basis for selection of chemotherapy in individual patients. A pooled analysis by Mandrekar et al.6 of 1053 patients with advanced-stage NSCLC undergoing first-line chemotherapy showed that gender, age, performance status, and hematologic parameters were significant predictors of severe adverse events. In another analysis, the incidence of grade 3 and 4 neutropenia was associated with advanced age (odds ratio = 7), low baseline white blood cell count (odds ratio = 5), and chronic hepatitis B or C virus infection (odds ratio = 3) in patients with advanced NSCLC undergoing second-line chemotherapy with docetaxel.7 Thus, clinical parameters such as performance status or age are commonly used by the practicing oncologist to decide which patients may not be suitable for standard chemotherapy approaches or who may need upfront dose reduction. On the other hand, when Borges et al.8 analyzed the potential predictive value of 22 clinical factors, including tumor histology, to predict tumor response following first-line chemotherapy in 1052 patients with NSCLC, none of the clinical factors accurately predicted response. Pursuing an alternative approach, Shaw et al.9 prospectively collected tumor tissue from 165 patients with NSCLC and SCLC, tested the chemosensitivity of tumor cells in vitro, and assigned individualized therapy based on these results. Despite efficient specimen collection (viable tumor specimens were available for 98% of the patients) and state-of-the-art culture methodology, only 28% of the patients received individualized chemotherapy based on laboratory results. This disappointing result precluded the comparison between treatment arms as well as the correlation between in vitro and clinical response to specific drugs. Although other groups have reported more optimistic results, in vitro drug sensitivity testing remains challenging and is not broadly accepted for clinical application at present.10,11,12
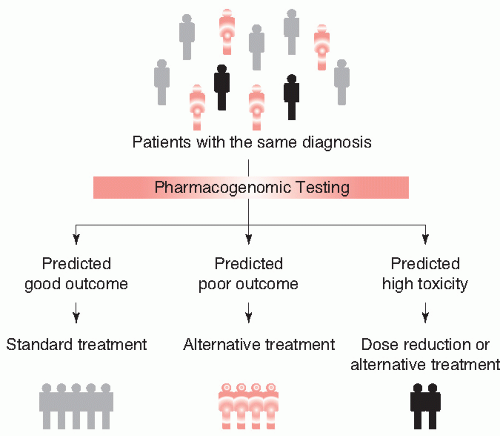
Conversely, a biomolecular approach to individualized chemotherapy, attempting to exploit individual patient differences in underlying tumor or host biology, is emerging as a more promising strategy for personalizing therapy (Fig. 47.1). The field of pharmacogenomics originated from the observation that inheritance plays an important role in individual variation in drug metabolism and disposition. In a broader sense, pharmacogenomics incorporates the entirety of molecular factors that modify drug activity and toxicity in individual patients. The development of this field occurred in parallel with recent advances in genomic science.13,14 Although the principle of individualizing chemotherapy for lung cancer patients is not new, the tools available to implement such an approach have previously been limited. Unfortunately, although clinical characteristics can give some insight into likelihood of response (i.e., the associations between female gender and good performance status with a higher response rate), they cannot reliably predict an individual patient’s response to chemotherapy. Similarly, past attempts at in vitro drug sensitivity testing have identified significant problems with the feasibility and reproducibility of this approach. Recent advances in genomic technologies and our understanding of the molecular mechanisms of chemotherapy, however, have brought forward several promising biomarkers with prognostic and/or predictive potential. Also, significant contributions toward a comprehensive understanding of the genetic variations underlying individual differences in drug metabolism have been made. In the near future, these advances are expected to impact on clinical decision making and ultimately improve the outcome of patients with lung cancer.
FIGURE 47.1 Concept of individualized chemotherapy. Activity and tolerability of chemotherapy varies among individual patients. Pharmacogenomic testing has the potential to predict who is likely to benefit from a specific drug (or drug combination) and who will have no benefit or may even be harmed by this treatment. Customized therapy may thus ultimately improve patient outcome.
In this chapter, two distinct aspects of pharmacogenomics are reviewed: (a) tumor-related factors including molecular drug targets that regulate the biochemical and physiological effects of drugs and their mechanisms of action and (b) hostrelated factors including metabolizing enzymes and transporters that regulate drug metabolism and disposition.
TUMOR-RELATED FACTORS: SINGLE-GENE BIOMARKERS
Biomarkers of Platinum Resistance The backbone of systemic treatment for both NSCLC and SCLC remains platinum-based chemotherapy.5,15 Among the platinum compounds, cisplatin (cis-diammine-dichloro-platinum, CDDP) is reported to have superior activity over carboplatin in NSCLC, in terms of response rate and, in patients with nonsquamous tumors, survival.16 The mode of action for cisplatin relates to the aquation equilibrium, a process by which a chloride ligand of cisplatin is displaced with water, allowing cisplatin to crosslink DNA via displacement of its second chloride ligand.17 The leaving ligand for carboplatin (cis-1,1-cyclobutanedicarboxylatodiammineplatinum[ II]) is bidentate cyclobutane dicarboxylate (CBDCA); whether there are consequences of this difference for biomarker development remains to be determined. Cross-linked DNA activates the nucleotide excision repair (NER) machinery, which includes a large complex consisting of at least 30 proteins, including ERCC1 (excision repair cross-complementing rodent repair deficiency, group 1), XPA (xeroderma pigmentosa group A), XPB/ERCC3, XPC, XPD/ERCC2, XPF/ERCC4, XPG/ERCC5, Cockayne syndrome protein A (CSA/ERCC8), CSB/ERCC6, and others (Fig. 47.2).18,19 If repair proves inadequate, NER triggers apoptosis. Thus, it is the balance between DNA damage and repair that determines the fate of cancer cells exposed to platinum. ERCC1, which forms a heterodimer with XPF, appears to be the rate-limiting step in NER, hence, its implication in platinum resistance. In preclinical models, ERCC1 levels correlated with the removal capacity of the cisplatin-induced DNA adducts as well as the relative cisplatin resistance.20,21,22 ERCC1-knockout cells were highly sensitive to DNA cross-linking agents, and transfection with ERCC1 exhibited an increase in the DNA repair capacity and cisplatin resistance.23,24
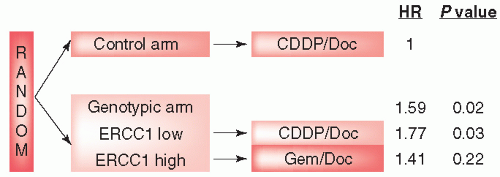
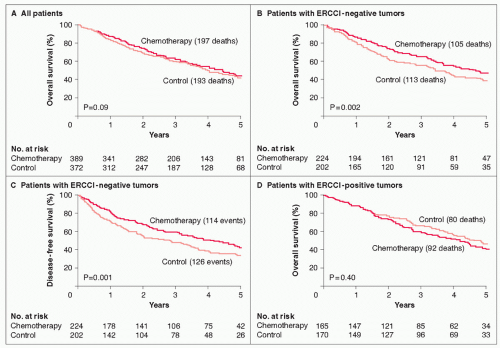
In view of these preclinical data, ERCC1 has emerged as an attractive single gene target in biomarker development for platinum-based chemotherapy. Indeed, clinical translation of these findings is highlighted by results in both advanced-stage NSCLC as well as in the adjuvant chemotherapy setting. In 2002, Lord et al.25 first reported that ERCC1 messenger RNA (mRNA) expression was significantly associated with response to cisplatin/gemcitabine chemotherapy in patients with advanced-stage NSCLC. The genomic international lung trial (GILT) of customized chemotherapy by the Spanish Lung Cancer Group also demonstrated the predictive value of ERCC1 for platinum-based chemotherapy but tested the role of nonplatinum chemotherapy as well.26 In this prospective phase III trial of individualized chemotherapy, 444 patients with previously untreated advanced NSCLC were randomized in a 1:2 ratio to either a control arm of docetaxel/cisplatin or a genotypic arm in which treatment was assigned based on the level of tumor ERCC1 mRNA expression, quantified by real-time reverse transcription polymerase chain reaction (RT-PCR). Patients in the genotypic arm, with tumors expressing ERCC1 mRNA levels lower than the median, received docetaxel plus cisplatin, whereas those with higher levels received docetaxel plus gemcitabine. With a significantly better response rate in the genotypic arm compared with the control arm (51.2% vs. 39.3%; p = 0.02), the study reached its primary end point. In multivariate analysis, low ERCC1 was an independent predictor of tumor response to cisplatin (Fig. 47.3). Neither median progression-free survival (PFS) (6.1 vs. 5.2 months; hazard ratio [HR] = 0.9; p = 0.30), nor overall survival (OS) was significantly different between the control and genotypic arm overall. However, there were interesting differences in outcomes between ERCC1-negative and – positive patients within the genotypic arm. Although response rates in the genotypic arm were relatively similar between ERCC1- negative patients treated with docetaxel/cisplatin (53%) versus the ERCC1- positive group receiving docetaxel-gemcitabine (47%), both PFS (6.7 vs. 4.7 months) and OS (10.3 vs. 9.4 months) were numerically higher in the ERCC1-negative group. These results suggest that although ERCC1-negative patients do well with platinum-based therapy, alternatives may be needed for the ERCC1-positive group, which extend beyond currently available nonplatinum regimens, such as that, used in this trial. The prognostic and predictive value of ERCC1 protein expression, assessed by immunohistochemistry, was reported by the International Adjuvant Lung Cancer Trial Biologic Program (IALT-Bio), a correlative science component of the IALT phase III trial testing adjuvant chemotherapy in early stage NSCLC reported (Fig. 47.4).27 The previously reported prognostic value of ERCC1 expression was confirmed in the control arm of IALT (surgery only), where ERCC1 positivity was associated with longer survival (HR = 0.66; 95% CI, 0.49 to 0.90; p = 0.009) compared with ERCC1 negativity. In the chemotherapy arm of IALT, only patients with ERCC1- negative tumors benefited from treatment (ERCC1-negative tumors: HR = 0.65; 95% CI, 0.50 to 0.86; p = 0.002), demonstrating the predictive value of this biomarker (ERCC1-positive tumors: HR = 1.14; 95% CI, 0.84 to 1.55; p = 0.40). These findings raise the question of whether patients with ERCC1-positive tumors would benefit from alternative therapies, such as nonplatinum-based chemotherapy regimens, or whether they would be best served by receiving no chemotherapy at all.
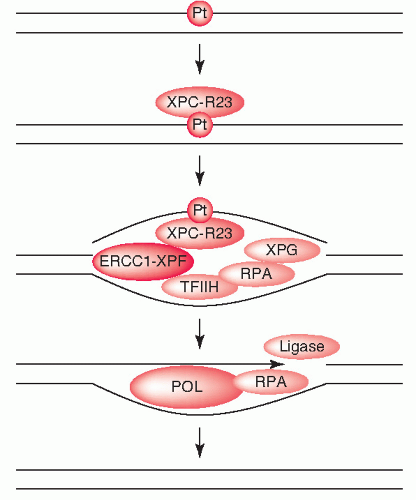
FIGURE 47.2 Molecular mechanisms of nucleotide excision repair (NER). DNA cross-linking by cisplatin (Pt) is recognized by XPC-R23, which recruits other proteins to form the active NER-complex. Only a few of these proteins are depicted here. For example, TFIIH unwinds the DNA, and ERCC1-XPF plus XPG cut out the damaged DNA strand. The gap is filled by polymerases (POL) and the ends are connected by ligases. These events restore the configuration of the damaged DNA strand. ERCC1, excision repair cross-complementing 1; POL, polymerase; RPA, replication protein A; TFIIH, transcription factor IIH; XP, xeroderma pigmentosum.
FIGURE 47.3 Genomic international lung trial (GILT). Trial design and results of the multivariate analysis for response according to tumor ERCC1 expression. See text for details. CDDP, cisplatin; Doc, docetaxel; ERCC1, excision repair cross-complementing 1; Gem, gemcitabine; HR, hazard ratio (for tumor response).
Ribonucleotide reductase M1 (RRM1) is the regulatory subunit of ribonucleotide reductase, which provides deoxyribonucleotides for de novo DNA synthesis and DNA repair. Gemcitabine, a nucleoside analogue that replaces cytidine during DNA replication, inhibits RRM1. High expression levels of RRM1 have been associated with gemcitabine resistance in NSCLC cell lines.28 Thus, RRM1 and ERCC1 may cooperate in resistance to platinum-based chemotherapy, especially platinum-gemcitabine combinations. In a study of 70 patients with advanced NSCLC, mRNA expression levels of ERCC1 and RRM1 (r = 0.624; p <0.001) were strongly correlated, and for the 33 patients treated with cisplatin plus gemcitabine, concomitant low levels of ERCC1 and RRM1 were predictive of better survival (14.9 vs. 10.0 months; p = 0.03).29 Bepler et al.30 in advanced NSCLC demonstrated that RRM1 mRNA expression correlated with tumor response from carboplatin plus gemcitabine. A prospective phase II trial (MADEIT) conducted by Simon et al.31 tested the feasibility and efficacy of patient selection for chemotherapy based on tumor ERCC1 and RRM1 mRNA levels. Median expression values were used to separate patients into four groups and patients were treated accordingly, with gemcitabine plus carboplatin (RRM1 low, ERCC1 low), gemcitabine plus docetaxel (RRM1 low, ERCC1 high), docetaxel plus carboplatin (RRM1 high, ERCC1 low), or docetaxel plus vinorelbine (RRM1 high, ERCC1 high). A median survival of 13.3 months was achieved, comparing favorably with previous results at the same institution and suggesting the clinical applicability of this approach. Zheng et al.32 used a newly developed fluorescence staining methodology for automated quantitative protein expression analysis (AQUA) to evaluate both ERCC1 and RRM1 protein in 187 patients with surgically resected NSCLC. RRM1 and ERCC1 expression were significantly correlated (r = 0.3; p = 0.001). With a median survival of 120 months, the 55 patients with concomitant high levels of RRM1 and ERCC1 lived significantly longer than other subgroups (p = 0.02). Based on the data reviewed previously, the Southwest Oncology Group will investigate the prognostic and predictive role of ERCC1 and RRM1 assessed by AQUA for adjuvant chemotherapy in patients with resected stage I NSCLC in a feasibility study, S0720.33 Patients with concomitantly high tumor levels of ERCC1 and RRM1 will receive no adjuvant chemotherapy, based on a good prognosis and predicted poor outcome from platinum chemotherapy, whereas all other patients will receive adjuvant chemotherapy with gemcitabine and cisplatin. Because adjuvant chemotherapy is not standard of care in stage I disease, this group is appropriate for such a study.34 The primary end point is feasibility, gauged by the percentage of patients in which a tumor specimen can be collected in a groupwide setting, assessed by AQUA, and results applied for treatment assignment.
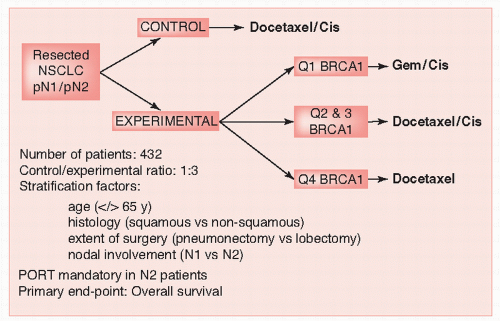
Another emerging factor in platinum resistance is BRCA1 (breast cancer 1, early onset). Although the involvement of BRCA1 in hereditary breast cancer and other malignancies is well known, other functions of this gene are still incompletely understood. A particular feature of BRCA1-deficient cells, as well as many cells showing a defect in homologous recombination, is sensitivity to the DNA cross-linking agents.35 In breast cancer cells, the absence of BRCA1 results in high sensitivity to cisplatin; conversely, BRCA1 expression increased sensitivity to antimicrotubule agents.36 Based on these findings, Taron et al.37 used real-time quantitative PCR (RTqPCR) to measure BRCA1 expression in 55 surgically resected tumors of patients with NSCLC who had received neoadjuvant gemcitabine/ cisplatin chemotherapy. In this study, patients with low BRCA1 expression levels had better outcomes than those with high levels. More recently, Rosell et al.38 studied the prognostic impact of BRCA1 expression in 126 specimens of resected early stage NSCLC. In this study, patients with high tumor expression of BRCA1 had significantly poorer survival. These results, taken together, led the Spanish Lung Cancer Group to initiate a pilot study of customized adjuvant chemotherapy based on BRCA1 mRNA levels in resected stage II to IIIA NSCLC patients, where adjuvant chemotherapy was customized based on BRCA1 mRNA levels in 84/100 completely resected N1 and N2 NSCLC patients. A total of 11 with high BRCA1 levels received docetaxel (doc); 29 patients with intermediate BRCA1 levels received doc/cisplatin (cis); 44 patients with low BRCA1 levels received cis/gemcitabine (gem). As of American Society of Clinical Oncology (ASCO) 2008, median survival had not been reached in patients with high or intermediate BRCA1 levels, although it was 25.6 months (m) in patients with low levels (p = 0.04). In a multivariate analysis for survival in all 84 patients, the HR were 5.23 for patients with high BRCA1 levels (p = 0.07) and 3.57 for patients with tumor size >4 cm (p = 0.07). In the multivariate analysis of 42 N2 patients, the HRs were 0.13 for 18 patients receiving postoperative radiotherapy (p = 0.04) and 22 for 15 patients with intermediate or high BRCA1 levels (p = 0.01). These interim analyses were interpreted to reveal that singleagent doc had no detrimental effect on survival in comparison with doc/cis. In addition, high BRCA1 mRNA expression could be a poor prognostic marker.39
FIGURE 47.5 Schema for the SCAT (Spanish customized adjuvant treatment in completely resected N1 and N2 non-small cell lung cancer) trial showing customized BRCA1 adjuvant treatment. See text for details. BRCA1, breast cancer 1; Cis, cisplatin; Gem, gemcitabine; NSCLC, non-small cell lung cancer; PORT, postoperative radiation therapy.
TABLE 47.1 Markers for Platinum Resistance in NSCLC
High p53 and greater survival benefit with chemotherapy
253
IHC
Modified from Gautschi O, Mack PC, Davies AM, et al. Pharmacogenomic approaches to individualizing chemotherapy for non-small cell lung cancer: current status and future directions. Clin Lung Cancer 2008;9(Suppl 3):S129-S138.
BRCA1, breast cancer 1, early onset; carb, carboplatin; cis, cisplatin; ERCC1, excision repair cross-complementing rodent repair deficiency complementation group 1; gem, gemcitabine; GILT, genomic international lung trial; IALT, International Adjuvant Lung Cancer Trial; IHC, immunohistochemistry; RTqPCR, reverse transcription quantitiative polymerase chain reaction; RRM1, ribonucleotide reductase M1; vin, vinorelbine.
Only gold members can continue reading. Log In or Register to continue