Fig. 1.1
The AESOP surgical system

Fig. 1.2
The Zeus surgical system
1.3 The da Vinci Surgical System
Frederic H. Moll, MD, a physician with a keen business sense saw the commercial value of the emerging robotic technology, acquired the license to the robotic surgical system pioneered by the NASA-SRI team, and started a company called Intuitive Surgical Inc.® in 1995. In January 1999, Intuitive launched the da Vinci Surgical System, which in 2000 became the first robotic surgical system accredited by the FDA for general laparoscopic surgery. In the following years, the FDA accredited the da Vinci Surgical System for thoracoscopic surgery, cardiac procedures performed with adjunctive incisions, urologic, gynecologic, pediatric and transoral otolaryngology procedures. The Intuitive Surgical Inc.® merged with Computer Motion, Inc.® in June of 2003, strengthening its intellectual property holdings [13].
The da Vinci Surgical System consists of three components: (1) surgical console, (2) patient cart, and (3) vision cart (Figs. 1.3, 1.4, and 1.5). The system provides the following advantages to the surgeons: three-dimension visualization, control of endoscopic instrument, and control of the camera. It enables direct real-time movement of endoscopic instrument by the operating surgeons and allows the surgeons to use techniques of open surgery during endoscopic procedures.



Fig. 1.3
The dual consoles of da Vinci Si at PLA General Hospital
Fig. 1.4
Patient cart
Fig. 1.5
Vision cart
The surgeon console is physically removed from the patient and allows the surgeon to sit comfortably (Fig. 1.6), resting the arms ergonomically while immersing himself/herself in the three-dimensional high-definition videoscopic image with the depth of the field through the view port. The surgeon controls the micro-instruments using the master controller. The medical signal, such as, ECG, oxygen saturation, and cardiac echo can be seen through stereo viewer in the surgical field (Fig. 1.7). Furthermore, various messages are displayed on the stereo viewer using icons and text. These enable the surgeon to monitor the status of the instruments and the arms without removing his/her head from the console.

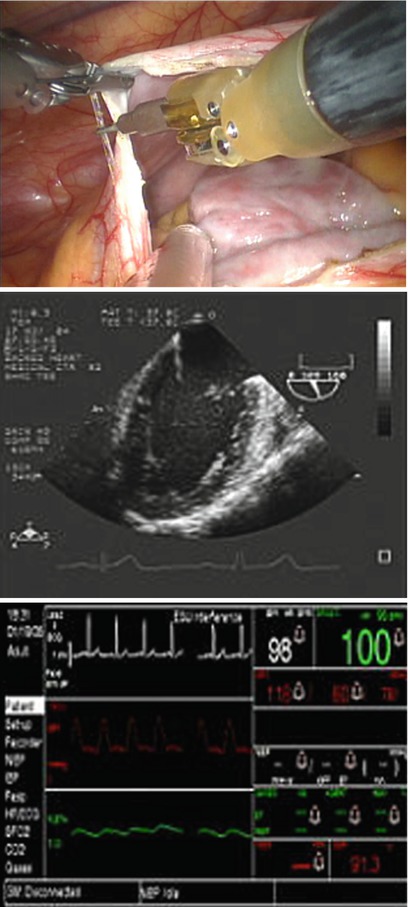
Fig. 1.6
The surgeon sits at the console at PLA General Hospital
Fig. 1.7
The medical signal can be seen through the stereo viewer during the surgery
The master controllers are used by the surgeon to control the instruments, the instruments arms, and the camera. The foot switches consists of instrument clutch, camera control clutch, camera focus, and electrocautery control. The armrest switches on the left and right armrests are used to control the motion and scaling of the robotic arms. And they are replaced by a touch screen panel in da Vinci Si Surgical System (Figs. 1.8 and 1.9).


Fig. 1.8
The surgeon console and its components of da Vinci S Surgical System
Fig. 1.9
A touch screen panel in da Vinci Si Surgical System replaces the traditional buttons at PLA General Hospital
Wrist and finger movements are digitally registered in computer memory, and then transferred to the instrument cart, where the synchronous end-effectors or micro instruments provide tremor-free movements with 7 degrees of freedom (Fig. 1.10). The instrument cart holds three arms in the first version (da Vinci®) and four arms in more recent models (da Vinci S® and da Vinci Si®) (Fig. 1.11). One arm supports the dual 5-mm diameter cameras to generate 3-D image and the other two or three arms are for wrist-like articulations equipped with EndoWrist Instruments that are designed to provide surgeons with natural dexterity and full range of motion.


Fig. 1.10
The “wrist” instrument provides the natural dexterity and full range of motion
Fig. 1.11
The four arms of da Vinci Si Surgical System docked at PLA General Hospital
The patient cart that rolls on wheels, is moved into the operative field, and is positioned over the patient. The robotic arms are designed like the human arm with a shoulder, an elbow, and a wrist. The instruments are attached to a carriage on the robotic arm. The carriage moves the instrument in and out a cannula at the tip of the arm. The cannula acts as the port that is introduced into the patient and carries the robotic instruments. The patient cart is connected with cables to the surgeon console.
The vision cart consists of the left eye camera control unit, right eye camera control unit, light source, video synchronizer and focus controller, assistant monitor, and various recordings and insufflation devices specific to the surgical application.
Using the most advanced technology available today, the da Vinci Surgical System enables surgeons to perform delicate and complex operations through a few tiny incisions with an increased vision, precision, dexterity and control.
1.4 Operating Room Configuration and System Setup
The da Vinci Surgical System consists of three main components: the Surgeon Console, the Patient Cart and the Vision Cart. The components should be arranged well in the operating room for maximum safety and ergonomic benefit (Fig. 1.12). The Surgeon Console is placed outside of the sterile field and is oriented where the Surgeon Console operator will have a view of the operative field and a clear line of communication with the Patient Cart operator (Fig. 1.12).

Fig. 1.12
The components of da Vinci Surgical System are arranged in the OR for clear communication at PLA General Hospital
The Patient Cart is draped prior to moving into place for surgery. The draped arms should be covered by an additional sterile coat (Fig. 1.13) to prevent coming into contact with non-sterile objects or impede traffic. Once the Patient Cart is draped, and the patient is positioned, prepared, draped and ports are placed, use the Patient Cart motor drive to help move the cart into the sterile field. The Vision Cart is placed adjacent to the Patient Cart, just outside of the sterile field, to allow the Patient Cart Operator to see the component displays (Fig. 1.14). The Vision Cart should be close enough to the Patient Cart to allow unrestricted camera cable movement during surgery.


Fig. 1.13
The draped arms are covered by an additional sterile coat to avoid contamination
Fig. 1.14
The Vision Cart is placed adjacent to the Patient Cart, to allow the Patient Cart Operator to see the component displays at PLA General Hospital
The components of da Vinci Surgical System are connected by three main cables. The three cables can be distinguished by their diameter and color. The cables should be arranged so that they are out of the path of OR traffic, including other equipment, to avoid damaging the cables or creating an obstacle or hazard.
Usually, a two-person team is assigned to handle non-sterile components: a scrub nurse and a circulating nurse drape the arms. The arms are draped systematically, allowing movement from left to right or right to left. Using the clutch buttons, the circulating nurse should move each straightened arm to provide plenty of room to maneuver around the arm. Once an arm is draped, the scrub nurse should move the draped arm away from the undraped arms and prepare to drape the next arm.
The preoperative management is critical to the success of robotic heart surgery. The patient should be positioned prior to docking the da Vinci Surgical system. The operating table should be easily moved prior to driving the Patient Cart into position. For robotic-assistant cardiac surgery, there are two opposite approaching routs, the left and the right chest walls. The surgical side of the patient’s chest is elevated at approximately 30° and with the arm tucked at the side (Figs. 1.15 and 1.16). Port placement is the key to a successful da Vinci procedure. The goals of port placement are to avoid Patient Cart arms collisions and maximize the range of motion for instruments and endoscope. The improper port placement may cause serious injury to the patient. Examples of port placement recommendations for cardiac surgery are provided in Figs. 1.6 and 1.7. Initial port location should be selected giving consideration to the procedure, specific anatomy, and the type of components being used.


Fig. 1.15
The patient position for right approach of da Vinci cardiac surgery with right side of the chest elevated at 30° and with the right arm tucked at the side
Fig. 1.16
The patient position for left approach of da Vinci cardiac surgery with left side of the chest elevated at 30° and with the left arm tucked at the side
Placement of the right ports: a 12-mm endoscopic trocar is placed into the right thoracic cavity through the incision made at 2–3 cm lateral to the nipple in the fourth intercostal space (ICS). A 1.5-cm incision is used as a working port in the same ICS for the patient-side surgeon. Additionally two 8-mm port incisions are made in the second and sixth ICS to allow insertion of the left and right instrument arms. The right instrument arm generally is positioned 4–6 cm lateral to the working port in the sixth ICS. The fourth arm trocar is placed in the midclavicular line in the 4th or 5th ICS (Fig. 1.17).
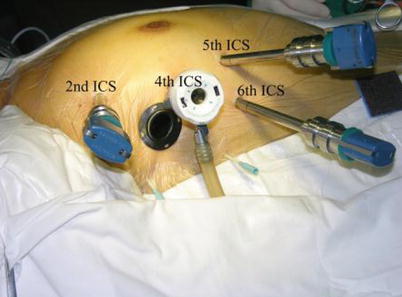
Fig. 1.17
Recommendatory ports placement for right approach of da Vinci cardiac surgery
Placement of the left ports: Three trocars were placed in the 3rd, 5th and 7th intercostal spaces that located about 3 cm lateral of the midclavicular line (Fig. 1.18).

Fig. 1.18
Recommendatory ports placement for robotic coronary artery bypass graft
Docking is the process of moving the Patient Cart up to the OR table and connecting the Patient Cart arms to the patient. Once the cannulas are inserted in the patient, the Patient Cart motor is moved into the sterile field (Fig. 1.19). Communication is critical when docking the Patient Cart. Use the instrument arm or camera port clutch button to bring the cannula mount to the cannula. If there are two instrument arms on one side, ensure that the instrument arm closest to the camera arm has adequate range of motion while minimizing collisions (Fig. 1.20).


Fig. 1.19
The Patient Cart is moved into the sterile field
Fig. 1.20
Instrument arm closest to the camera arm has adequate range of motion
1.5 Robotic Cardiac Surgery
Cardiac surgery has been conventionally performed via median sternotomy for the convenience of adequate exposure and surgeons’ generous access to the heart and surrounding vessels. Since the notion of minimally invasive surgery was introduced to cardiovascular surgery, surgeons are keen on developing less invasive methods without any compromise on accessibility and dexterity thus resulting in paradigm shift in cardiac surgery. With the application of surgical robotic systems, surgeons are enabled to improve dexterity and perform ambidextrous sutures in the limited space. The procedures have hitherto been successfully performed such as mitral valve reconstruction and replacement, coronary revascularization, atrial fibrillation surgery, left ventricular lead placement, intra-cardiac tumor resection, congenital surgery, etc.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


