Percutaneous Balloon Mitral Commissurotomy, Mitral Repair, and Pulmonic, Tricuspid, and Aortic Valvuloplasty
Percutaneous Balloon Mitral Commissurotomy, Mitral Repair, and Pulmonic, Tricuspid, and Aortic Valvuloplasty
Ted Feldman MD, FESC, FACC, FSCAI
Alice Perlowski MD
Although percutaneous techniques for the treatment of structural heart disease represent revolutionary technology, the basic principles of these therapies were born from concepts developed several years ago. For example, pulmonic valve stenosis was treated with percutaneous catheter therapy as early as the 1950s (1). Balloon valvuloplasty was first described in 1982 by Inoue, and has subsequently developed into a mature therapy for mitral, pulmonic, and aortic stenosis (2, 3 and 4). This chapter reviews percutaneous valvuloplasty as it is practiced today and provides an overview of the next horizon in catheter valve therapy: percutaneous mitral valve repair and replacement.
BALLOON COMMISSUROTOMY FOR MITRAL STENOSIS
Rheumatic heart disease is an infrequent diagnosis in the United States, but remains an important diagnostic entity. Immigrants have entered the United States from all over the world, importing rheumatic heart disease from Mexico, Asia, and Central and South America (5). Also, new strains of Streptococci have been associated with rheumatic fever in the United States, and streptococcal skin and kidney infections have been implicated in some outbreaks of rheumatic disease (6).
It is important to recall that initial attacks of rheumatic fever require specific therapy. The rheumatic disease process not only attacks the valves but also produces a pancarditis, which may adversely affect atrial and ventricular function. Atrial fibrillation in association with rheumatic mitral stenosis is probably caused by both left atrial distention and damage to the atrial tissue at the time of the acute rheumatic infection. Mitral stenosis is synonymous with rheumatic valve disease. Etiologies other than rheumatic are encountered rarely. Congenital mitral stenosis, carcinoid, and eosinophilic endomyocardial fibroelastosis represent rare causes of mitral stenosis. Increasingly, calcific mitral stenosis in association with severe mitral annular calcification or among patients on chronic hemodialysis is being recognized.
It is critically important to recognize the difference between calcific and rheumatic disease. The hallmark of rheumatic mitral stenosis is commissural fusion, usually in association with subvalvular thickening, and with involvement of aortic, tricuspid, and/or pulmonic valves. A typical chronic calcific patient has calcification extending from the annulus toward the body of the leaflets with free movement of the leaflet tips, little involvement of the chordae, and no evidence for commissural fusion. Clinical history is critical for the diagnosis of mitral stenosis. The sine qua non of the disease is dyspnea on exertion. Patients may be misdiagnosed with a history of asthma or other lung diseases. Some patients have even had lung biopsy for a long-standing diagnosis of interstitial disease until pulmonary congestion from rheumatic mitral stenosis is diagnosed. Exercise intolerance and dyspnea develop in almost all patients with clinically significant disease. With exercise, cardiac output rises with a disproportionate increase in the left atrial and pulmonary artery pressures.
TABLE 40-1 Mitral Valve Score
Mobility
Subvalvular
Thickening
Calcium
1
Tips restricted
Minimal thickening
normal ??????(4-5 mm)
Single area
2
Mid and base normal
1/3 chordal length
Leaflet margins 5-8 mm
Scattered
3
Valve moves forward
Thick to distal chords
Entire leaflet 5-8 mm
Mid-leaflets
4
Barely mobile
Extensive to paps
>8-10 mm thick
Extensive
From: Wilkins GT, et al. Br Heart J. 1988;60:299-308, with permission.
Many patients with mitral stenosis adamantly deny any limitation in exercise tolerance. Patients often decrease their activity level to avoid symptoms. This history requires some effort to elicit. Exercise testing can be helpful when the symptomatic status of a patient is not clear (7). In particular, serial exercise testing over a period of several years is often very helpful when a patient presents with moderate disease initially.
Echocardiographic Evaluation
Transthoracic echocardiography is the primary tool for assessment of patients for suitability for balloon mitral commissurotomy (BMC).A scoring system has been described that utilizes four characteristics to characterize the spectrum of mitral valve deformity (Table 40-1) (8). The score combines descriptions of leaflet mobility, leaflet thickening, calcification, and subvalvular involvement on a scale, where 1 is minimal deformity and 4 represents severe deformity. The scoring system is relatively subjective and has a large amount of interobserver variability. Despite the limitations, it represents a common currency for describing the degree of valve deformity and mitral stenosis. Scores of 8 or less have been associated with excellent long-term results from BMC, while scores >12 have poor long-term outcomes and high incidence of mitral regurgitation complicating the procedure. Echocardiographic scores between 9 and 12 are associated with intermediate long-term outcomes. Patients with lower echo scores have event-free survival rates over 5 years after BMC exceeding 80%. The event-free rate over 5 years declines to about 60% among those with intermediate scores. Patients with severe valve deformity are usually poor candidates for any form of therapy and receive BMC as a palliative therapy when the risk of surgery is prohibitive. These patients typically present at a later age in states of advanced disease, and have poor long-term outcomes.
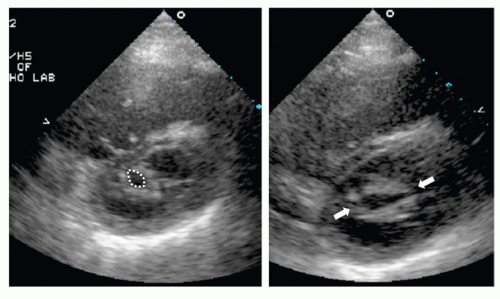
FIGURE 40-1 The left-hand panel shows a short-axis transthoracic echocardiographic image at the level of the mitral valve orifice. Planimetry of the orifice shows the typical fishmouth appearance (dotted circle). The interventricular septum is flattened due to chronic pulmonary hypertension. There is dense, symmetrical commissural fusion. On the right, after balloon mitral commissurotomy, there is bilateral commissural splitting, shown by the white arrows. The interventricular septum is now more round, consistent with immediate diminution of the pulmonary artery pressure.
The short axis transthoracic echo view can be used to assess the symmetry of commissural fusion (Fig. 40-1). Symmetric commissural fusion and the absence of leaflet calcification are associated with the best balloon dilatation results. Asymmetric fusion and/or calcification of the commissures typically yield less optimal results from balloon dilatation because of the reduced ability of the balloon to split the commissures in a controlled, predictable fashion.
TABLE 40-2 Indications for Coronary Arteriography for Patients with Valve Disease
Class I
1. Coronary angiography is indicated before valve surgery (including infective endocarditis) or mitral balloon commissurotomy in patients with chest pain, other objective evidence of ischemia, decreased LV systolic function, history of CAD, or coronary risk factors (including age).
Patients undergoing mitral balloon valvotomy need not undergo coronary angiography solely on the basis of coronary risk factors. (Level of Evidence: C)
2. Coronary angiography is indicated in patients with apparently mild to moderate valvular heart disease but with progressive angina (Canadian Heart Association functional Class II or greater), objective evidence of ischemia, decreased LV systolic function, or overt congestive heart failure. (Level of Evidence: C)
3. Coronary angiography should be performed before valve surgery in men aged 35 years or older, premenopausal women aged 35 years or older who have coronary risk factors, and postmenopausal women. (Level of Evidence: C)
Class IIa
1. Surgery without coronary angiography is reasonable for patients having emergency valve surgery for acute valve regurgitation, aortic root disease, or infective endocarditis. (Level of Evidence: C)
Class IIb
1. Coronary angiography may be considered for patients undergoing catheterization to confirm the severity of valve lesions before valve surgery without pre-existing evidence of CAD, multiple coronary risk factors, or advanced age. (Level of Evidence: C)
Class III
1. Coronary angiography is not indicated in young patients undergoing nonemergency valve surgery when no further hemodynamic assessment by catheterization is deemed necessary and there are no coronary risk factors, no history of CAD, and no evidence of ischemia. (Level of Evidence: C)
2. Patients should not undergo coronary angiography before valve surgery if they are severely hemodynamically unstable. (Level of Evidence: C)
From: Bonow RO, et al. J Am Coll Cardiol. 2008;52:e1-e142, with permission.
Coronary arteriography is indicated prior to BMC for patients with chest pain or evidence of ischemia, poor left ventricular function, history of coronary artery disease, for male and postmenopausal female patients over the age of 35 years, and in premenopausal female patients when risk factors for coronary artery disease are present (Table 40-2) (9).
Patient Selection
BMC has become the therapy of choice for the majority of patients with symptomatic mitral stenosis (Table 40-3) (9).BMC is recommended for symptomatic patients with a valve area of <1.5 cm2 who have favorable valve morphology, no left atrial thrombus, and no severe mitral regurgitation. Treatment for asymptomatic patients is challenging. Those who have no symptoms and a mitral valve area of <1.5 cm2 may be considered for catheter commissurotomy if the pulmonary artery systolic pressure is >50 mm Hg at rest or 60 mm Hg after exercise. New atrial fibrillation has also been defined as an indication for BMC in patients without symptoms. Patients with moderate to severe mitral stenosis (MS) and New York Heart Association (NYHA) Class 3 or 4 symptoms, who have restricted, nonpliable calcified leaflets and are at high risk for mitral valve surgery, are also good candidates for BMC (Class IIa).
TABLE 40-3 Indications for Balloon Mitral Commissurotomy
Class I
1. BMC is effective for symptomatic patients (NYHA functional Class II, III, or IV), with moderate or severe MS and valve morphology favorable for BMC in the absence of left atrial thrombus or moderate to severe MR. (Level of Evidence: A)
2. BMC is effective for asymptomatic patients with moderate or severe MS and valve morphology that is favorable for BMC who have pulmonary hypertension (pulmonary artery systolic pressure >50 mm Hg at rest or >60 mm Hg with exercise) in the absence of left atrial thrombus or moderate to severe MR. (Level of Evidence: C)
Class IIa
1. BMC is reasonable for patients with moderate or severe MS who have a non-pliable calcified valve, are in NYHA functional Class III-IV, and are either not candidates for surgery or are at high risk for surgery. (Level of Evidence: C)
Class IIb
1. BMC may be considered for asymptomatic patients with moderate or severe MS and valve morphology favorable for percutaneous BMC who have new onset of atrial fibrillation in the absence of left atrial thrombus or moderate to severe MR. (Level of Evidence: C)
2. BMC may be considered for symptomatic patients (NYHA functional Class II, III, or IV) with mitral valve (MV) area greater than 1.5 cm2 if there is evidence of hemodynamically significant MS based on pulmonary artery systolic pressure >60 mm Hg, pulmonary artery wedge pressure of 25 mm Hg or more, or mean MV gradient >15 mm Hg during exercise. (Level of Evidence: C)
3. BMC may be considered as an alternative to surgery for patients with moderate or severe MS who have a nonpliable calcified valve and are in NYHA functional Class III-IV. (Level of Evidence: C)
Class III
1. BMC is not indicated for patients with mild MS. (Level of Evidence: C)
2. BMC should not be performed in patients with moderate to severe MR or left atrial thrombus. (Level of Evidence: C)
From: Bonow RO, et al. J Am Coll Cardiol. 2008;52:e1-e142, with permission.
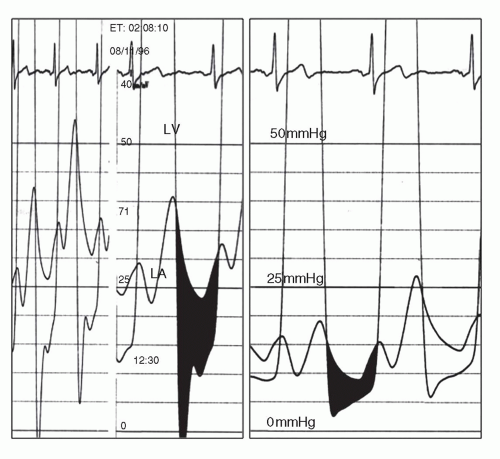
FIGURE 40-2 Simultaneous left atrial (LA) and left ventricular (LV) pressures before and after BMC. On the left, the shaded area shows a large transmitral pressure gradient. On the right, immediately after BMC, the gradient has been reduced. The left atrial waveform remains unchanged, with no increase in the “V” wave, indicating that this result has been achieved without any significant worsening of mitral regurgitation.
Acute Results and Complications
The hemodynamic results of BMC have been consistent regardless of the method used for the procedure (10). The immediate intra-procedure results are dramatic (Fig. 40-2). There is a decline of left atrial pressure and transmitral pressure gradient with an associated increase in cardiac output and consequently, an increase mitral valve area. In patients with hypertensive heart disease or left ventricular (LV) diastolic pressure elevations, the diminution in gradient may be overshadowed by persistently high ventricular diastolic and left atrial pressures. On average, the mitral valve area increases from 1.0 cm2 to between 1.8 and 2.2cm2. Pulmonary hypertension typically decreases by between 10% and 25% as soon as the valve has been opened. Immediate declines in left atrial and pulmonary artery pressure often lead patients to spontaneously note improvement in their sense of breathing while they are still on the cardiac cath lab table. Additional decreases in pulmonary pressure usually take place over the several weeks or months after procedure (11). Despite these improvements, severe pulmonary hypertension usually does not completely resolve. Atrial fibrillation reverts in only 20% to 25% of patients. This is probably because of rheumatic involvement of the atria and the persistent fibrosis of atrial tissue caused by chronic left atrial distension.
The most important complication of BMC is an increase in mitral regurgitation. About 2% to 3% of patients require mitral valve replacement during the hospitalization for the procedure. As many as one-third of patients have an increase in mitral regurgitation associated with a net benefit in clinical outcome. Intraprocedural or hospital death occurs in <1% of patients.
BMC-related stroke or transient ischemic attack as a consequence of embolization from the left atrial appendage has been virtually eliminated by the routine use of transesophageal echo as a preprocedure screening tool. The incidences of these complications are similar to other catheterization procedures. Cardiac perforation associated with transseptal puncture occurs in about 1% in most series. Perforation of the ventricle by the balloon is rare with the Inoue Balloon, and is more frequent with the longer, sharper tipped double balloons.
Most techniques for BMC involve transseptal puncture, with creation of an atrial septal defect (12). Color flow Doppler demonstrates shunt flow in almost all patients immediately after procedure, but most atrial septal defects close spontaneously within a few weeks or months. Less than 2% of patients have atrial septal shunting, with shunt ratios >1.5. Persistent shunting is often related to suboptimal left atrial decompression and persistently elevated left atrial pressure, which maintains left to right intraatrial flow.
Long-term Outcome
After 5 years, about 70% of patients remain event-free following BMC. The subgroups of patients with more or less pliable valves have significantly different results. The ideal patient with little valve deformity has a 5-year event-free survival rate that exceeds 80%, while older patients with severe valve and subvalvular deformity may have a 5-year event-free survival closer to 50%. For these older patients, achieving the optimum, durable hemodynamic result is less important, and palliation is the goal of therapy.
An important consideration in assessing the outcomes after BMC is the patient population that is being described. The country from which a report originates is critical to understanding differences in reported procedure outcomes. Patients from the United States undergoing BMC have a mean age of around 55 years. In contrast, reports from Asia describe populations with mean age of 25 to 35 years, and those from India, an even younger population. The course of rheumatic disease differs greatly among these different demographic and age groups. It is critical to understand the differences in specific populations to adequately assess whether surgery or a particular percutaneous approach might be optimal in a given clinical setting. Thus, comparisons among structural heart trials performed in different geographic areas must be made with great caution.
Randomized trials are the only acceptable manner to compare surgical commissurotomy with BMC. Randomized comparisons of balloon and surgical commissurotomy have shown that the two approaches are equivalent (13). The hemodynamic and valve area results in these trials have been reported with up to 10-year follow-up (14).
Only gold members can continue reading. Log In or Register to continue
May 28, 2016 | Posted by drzezo in CARDIOLOGY | Comments Off on Percutaneous Balloon Mitral Commissurotomy, Mitral Repair, and Pulmonic, Tricuspid, and Aortic Valvuloplasty