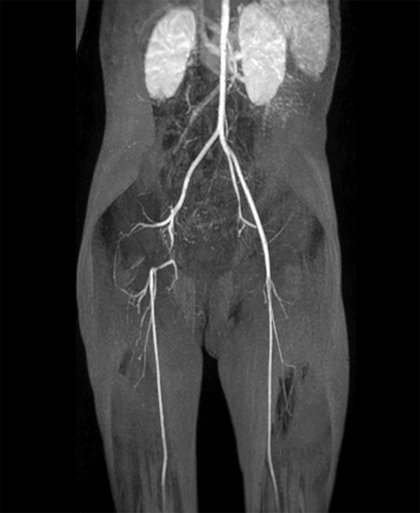
An open revascularization may become necessary if limb-threatening ischemia exists or progressive ischemic injury occurs. Resection and primary repair may be possible in cases of a very focal occlusion. Interrupted sutures with spatulation of the involved vessels, so as to create ovoid anastomoses, will lessen the risk of later narrowing at the anastomosis. A small vein patch may be used if a primary arterial repair is precluded by the extent of the injury. Long-term follow-ups of vein patches have not been reported, although small case series with short-term follow-up support this option. More extensive injuries can require bypass with reversed saphenous vein (Figures 1 and 2). Late aneurysmal deterioration of such vein grafts used in reconstructing extremity arteries occurs less often than when they are used for renal arterial reconstructions. Nevertheless, long-term follow-up of any vein graft (or patch) in children is mandatory. Late vein graft failure as a result of neointimal hyperplasia or thrombosis has been reported in 5% of patients. If these injuries are managed nonoperatively and the occlusion does not recanalize, or if collateral circulation is ultimately insufficient, then certain subtle complications can ensue. These include complaints of pain with ambulation and potential retardation of long-bone growth with subsequent limb length discrepancies and gait abnormalities. Limb length discrepancy is not a rare occurrence following arterial catheterization in young patients, and length disparity rates of 8% are reported following femoral artery access in children 5 years old or younger. These events often go unrecognized as a result of the development of extensive collaterals, restoring palpable pulses in the affected extremity (Figure 3).
Pediatric Iatrogenic Vascular Injury
Lower Extremity and Femoral Artery

![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine