Chapter 14
Patient Clinical Evaluation
Philip P. Goodney
Based on a chapter in the seventh edition by G. Matthew Longo and Thomas G. Lynch
The emphasis of this chapter is on the use of the history and physical examination to identify the various disease states associated with arterial, venous, and lymphatic pathology. In general, the lower extremities provide a model for the clinical evaluation of patients with peripheral vascular disease and can be used to demonstrate the value of an organized approach to the history and physical examination. When appropriate, correlation will also be made with related pathology and symptoms in the upper extremities.
Overview
First, the patient’s chief complaint should be determined; the physical examination should be correlated with the history and should also provide a bridge to the pathophysiology of the disease process.1,2 As an example, aortoiliac obstructive disease will often be associated with more proximal symptoms of claudication involving the buttock, hip, or thigh. If the clinical history is accurate, the examiner should expect that the femoral pulse will be absent or decreased. If the history is not accurate, the history and assumptions regarding pathophysiology should be questioned.
When the history and physical examination are completed, diagnostic studies can be ordered, if necessary, to further localize the disease or quantify the extent of the process. Therapy is ultimately driven by the natural history of the disease process and its impact on quality of life, as well as by the patient’s risk factors and functional status. A relatively benign natural history or significant and unmodified patient risk factors may indicate an initial course of medical management, risk factor modification, and observation, whereas threat of tissue loss may indicate a need for more aggressive intervention.
Evaluation begins with identifying the patient’s signs and symptoms. It is important to obtain a chronologic description of the development and progression of the patient’s main complaint from the first sign or symptom to the present.
Clinical History
Typically, the symptoms of arterial and venous disease can be broadly classified into the following categories: pain; weakness; neurosensory complaints, including warmth, coolness, numbness, and hypersensitivity; discoloration; swelling; tissue loss and ulceration; and varicosities. Critical elements include the initial onset of symptoms (acute or chronic); progression or changes since the initial onset; location (unilateral, bilateral, proximal, distal); character or quality of the symptom or complaint; some measure of the extent of disability or limitation; the context or factors precipitating or aggravating the symptoms (activity, position, temperature, menses, vibration, pressure); factors mitigating or relieving symptoms; and associated signs, symptoms, or risk factors. In the assessment of vascular disease, the history is important. As will be seen, variations from the expected history or pattern of findings may suggest additional disease processes that may be included in the differential diagnosis.
As part of the history, associated vascular disease and predisposing risk factors should also be identified. Atherosclerotic vascular disease is a systemic process. A patient with claudication may also have a history of coronary artery disease or stroke. Predisposing risk factors for arterial disease can include hypertension, hyperlipidemia, diabetes, chronic renal insufficiency, and a history of smoking. Venous disease can be associated with obesity, immobility, cancer, trauma, hypercoagulability, and a history of deep venous thrombosis.
Physical Examination
The physical examination links the clinical history and the pathophysiology of the arterial, venous, or lymphatic disease process. The pathology associated with arterial disease can be broadly classified into inflammation-mediated arterial wall changes, arterial wall irregularity or ulceration, stenosis and/or occlusion, and dilatation and aneurysmal degeneration. Veins are normally patent and competent, with functioning valves. Pathologically, intraluminal thrombus can partially or completely obstruct veins. With recanalization of thrombus, veins can become incompetent and lose their valvular function. Valvular incompetence can also develop primarily, independent of previous thrombosis. Finally, if flow through the lymphatic system is disturbed by obstruction, compression, or absence of the lymphatic channels, lymphedema may result.
The physical examination should progress from inspection, to palpation, to auscultation. On inspection, the extremity should be assessed for evidence of skin changes, including atrophy, cyanosis or mottling, pallor, and rubor; hair distribution; and abnormalities in nail growth. The presence and location of edema should be identified and quantified. Tissue loss and ulceration should be noted and fully described, including the location, size, and depth, and the presence of associated cellulitis and inflammation should be documented. Motor function should be documented. On initial palpation, changes in temperature and sensation should be noted and compared with the contralateral extremity. All accessible pulses should be evaluated. At a minimum, pulses should be classified as absent, decreased, or normal. A prominent or widened pulse may suggest aneurysmal degeneration.
Synthesis of the History and Physical Examination
Assessment of a patient with vascular disease is unique, in that it is frequently possible to make a diagnosis and predict the underlying anatomic pathology on the basis of history and physical examination alone. This is important because the anatomy of the disease process can often correlate with the location of symptoms. The history and physical examination should be thought of as a system of checks and balances. Symptoms should correlate with the physical examination and suspected pathology. Such correlation is important because additional evaluation and invasive assessment may not be critical to the initial treatment if the anatomic pathology can be inferred from the history and physical examination.
Arterial Disease—History
Patients with peripheral arterial disease (PAD) may initially be seen after acute arterial occlusion or with symptoms of chronic arterial insufficiency. Regardless of whether the onset of symptoms is acute or chronic, the chief complaint is generally pain or discomfort. As part of the initial history, it is important to determine the acuteness of onset, the character and intensity of the pain or discomfort, changes in the character and intensity since onset, and its location.
Acute Arterial Occlusion
Acute arterial occlusion may be either embolic or thrombotic in etiology. Classically, acute arterial occlusion is associated with the six “Ps”: pain, pallor, pulselessness, paresthesias, paralysis, and poikilothermy (meaning changing to room temperature, i.e., a cold extremity). Symptoms can occur within minutes to hours after acute arterial occlusion and are associated with a sudden, dramatic decrease in perfusion. Classically, a patient will complain of generalized pain that is severe and not well localized. The patient will notice a change in the color of the extremity, a decrease in sensation, and coolness to touch. Absent motor function is consistent with severe limb-threatening ischemia. An improvement in symptoms over time suggests the development of collateral circulation after the acute arterial occlusion, whereas progression of symptoms suggests lack of collateralization and increasing ischemia.
Acute Arterial Occlusion of the Lower Extremity
As a rule, patients with acute arterial occlusion secondary to an embolic etiology will not have a history of claudication or symptoms suggestive of chronic occlusive arterial disease. Embolic occlusion of the iliac, femoral, or popliteal arteries is frequently associated with a history of atrial fibrillation, and the patient may have had a previous embolic event. In patients who are normally on a regimen of long-term anticoagulation, warfarin (Coumadin, Bristol-Myers Squibb, Princeton, NJ) may have recently been discontinued before a planned intervention, or the patient’s international normalized ratio may have been subtherapeutic. Patients with thrombotic occlusion of the iliac, femoral, or popliteal arteries will frequently have a history of claudication and may have previously undergone arterial bypass or intervention.
Atheroembolism: “Blue Toes Syndrome”
Atheroembolic debris arising from atherosclerotic plaque or ulcerations in the aorta, as well as the iliac, femoral, and popliteal arteries, can result in distal small arterial occlusion. Progressive renal insufficiency can be associated with atheroemboli originating in the thoracic or suprarenal aorta. Patients often have undergone some form of catheter-based procedure involving manipulation of a catheter in the aortic arch or the thoracic and abdominal aorta, or the embolism may be spontaneous.
Distal emboli or thrombotic occlusion can also be due to peripheral arterial aneurysms. Patients will have a painful bluish discoloration of the distal part of the foot or digits, resulting in “blue toe syndrome.” Calf pain can be associated with focal areas of ischemia or tissue necrosis. Symptoms are generally sudden in onset and slow to resolve. The patient often notes that the involved foot or digit feels cool and numb to touch.
Acute Arterial Occlusion of the Upper Extremity
Although less common, acute arterial occlusion may also occur in the upper extremities. The onset and symptoms are similar to those seen in the lower extremities. Emboli associated with atrial fibrillation or recent myocardial infarction are more common but may also originate from aneurysmal disease of the arch or upper extremity arteries. Atheroemboli involving the hand or digits may arise from atherosclerotic irregularity and plaque in the aortic arch or from thrombus associated with a subclavian artery aneurysm. Thrombotic events are infrequent, but may be associated with subclavian artery aneurysms.
Chronic Obstructive Arterial Disease
Patients with peripheral arterial disease (PAD) most commonly have long-standing symptoms. Chronic occlusive arterial disease encompasses a spectrum of symptoms, beginning with effort discomfort (claudication) and progressing to pain at rest and tissue loss.3 Claudication is derived from the Latin word claudicatio, which means to limp or be lame. Thus, claudication involves the lower extremities and is associated with walking. Effort-induced discomfort with activity involving the upper extremity can be associated with stenosis or occlusion of the subclavian and axillary arteries.4
To ease communication between health care professionals who care for patients with PAD, many have adopted the Rutherford classification as the preferred clinical staging system.5 Although it is described in greater extent in other chapters (see Chapters 108 and 109), this clinical staging system ranges from asymptomatic (stage 0), to mild or moderate claudication (stage 3), to severe (stage 6). An example of a patient with stage 0 Rutherford classification would be an elderly patient with a low ankle-brachial index, but no findings of claudication or critical limb ischemia, whereas a patient with Rutherford stage 6 ischemia has severe ulceration and gangrene, as a result of rapidly impending limb-threatening ischemia. The clinical presentation of these entities is described in the following.
Lower Extremity Claudication
Patients with claudication will describe symptoms that are associated with walking. Because the symptoms are secondary to inadequate or decreased circulation, relief occurs promptly after the cessation of activity. Complete relief of symptoms should occur within 5 to 10 minutes, and it should not be necessary for the patient to sit to obtain relief. The exercised-induced symptoms can be described as cramping, aching, fatigue, or numbness; the common denominator is an association with exercise or activity.
Symptoms may have been present for months or years. Anatomically, lower extremity PAD is broadly classified as aortoiliac, femoropopliteal, or tibial. Depending on the location of the arterial obstruction, the patient may have pain in any of the three major muscle groups of the lower extremity: the buttock, thigh, or calf. Symptoms may involve one or more of these muscle groups and may progress from the proximal to the distal part of the extremity or from the calf to the thigh with continued activity. Symptoms will often occur in the muscle group immediately distal to the obstruction. Although obstruction of the superficial femoral artery will cause calf discomfort, aortoiliac disease will result in symptoms involving the buttock or thigh. However, patients with aortoiliac disease can also have associated or isolated discomfort of the calf because the calf is the most distal large muscle group and is used extensively in walking. The triad of intermittent claudication, impotence, and absent femoral pulses is associated with aortoiliac occlusion and is often referred to as Leriche syndrome. In his initial descriptions of the disease process, Leriche et al6 also identified widespread atrophy of the lower extremities and a pale appearance of the extremities and foot.
The severity of symptoms or the extent of disability is usually quantified relative to the distance that a patient can walk or flights of stairs that can be climbed before it is necessary to stop and rest. Usually exercise tolerance deteriorates when walking up a hill or an incline because greater energy expenditure is required than when walking on level ground.
Some patients with PAD confirmed by noninvasive vascular testing may not complain of claudication because comorbid conditions may limit their exercise tolerance. Conversely, other patients may have classic symptoms of claudication but a normal pulse examination. Because initial assessment generally occurs while the patient is at rest on the examining table, it is important to remember that the claudication occurs with walking. In cases when there is a mismatch between the history and physical examination, the physical examination may need to be repeated after exercise.
Conditions Mimicking Arterial Claudication
Classically, claudication is associated with arterial stenosis or occlusion, is induced by exercise and relieved by rest, and has an onset that is consistently reproducible. Inconsistencies in the history should suggest the possibility of other causes of the patient’s symptoms. Included in the differential diagnosis of claudication are musculoskeletal, neurologic, and venous pathologies, the most common of which are osteoarthritis, spinal stenosis, and venous outflow obstruction. Symptoms that occur at rest, occur with standing, or are associated with positional changes may suggest osteoarthritis, spinal stenosis, radiculopathy, or venous claudication (Table 14-1).
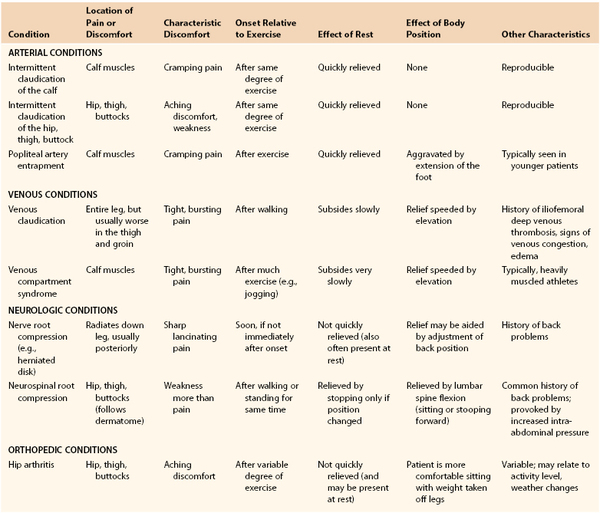
Patients with atypical claudication of nonarterial etiology will often note pain with exertion, yet the pain does not stop the individual from walking, may not involve the calves or other major muscle groups in the leg, or does not resolve within 10 minutes of rest.7–9 Patients may report the same type of pain in both legs regardless of the associated presence of occlusive disease. Frequently, patients with atypical symptoms often report walking impairment because of joint pain or shortness of breath.7,8
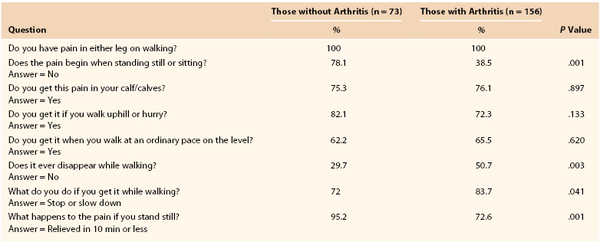
Ultimately, in the evaluation of an individual with leg pain, the examiner has to be cognizant of the patient’s comorbid conditions in an effort to offer the most complete treatment. Newman et al8a compared answers to the Rose Questionnaire in patients with and without arthritis, all of whom had a decreased ankle-brachial index and exertional leg pain. Both groups had pain in the calf or calves on walking at a normal pace, while in a hurry, or when walking uphill. The patients with arthritis, however, had a higher incidence of pain when standing still or sitting, were less likely to continue walking after the onset of pain, and required more than 10 minutes to obtain relief after they had stopped walking (Table 14-2).
Several previous reports have examined the sensitivity and specificity of the Rose Questionnaire for patients with intermittent claudication. Geoffrey Rose at the London School of Hygiene designed the original questionnaire, which was used to identify patients with intermittent claudication.10 Although the original questionnaire was highly specific (>90%), it was not very sensitive (<70%). Several investigators, including those described previously, have worked to refine the sensitivity of this instrument and others like it. These tools are critical in attempts to discern patients with and without significant claudication from those with other conditions that cause leg pain.
Neurogenic Claudication.
Neurogenic claudication due to spinal stenosis can result from a wide range of conditions causing compression of the spinal cord or its nerve roots in the region of the lumbar spine. It may be associated with aging, arthritis, or inherited deformities of the spine. The symptoms of spinal stenosis are frequently inconsistent in their relationship to exercise or activity. It is not unusual for patients to be limited in their activity one day and be relatively symptom free the next. After the onset of symptoms associated with spinal stenosis, relief does not occur promptly once activity has ceased. Complete symptomatic relief may take 30 to 60 minutes or longer. Commonly, the patient will have to sit down or lean forward. Leaning forward flattens or straightens the lumbar lordosis and often relieves the cord compression.
Venous Insufficiency and/or Venous Claudication.
In an individual with venous claudication, symptoms are associated with a proximal venous obstruction resulting in impaired venous outflow. When an individual begins to exercise or engage in some activity, venous outflow cannot accommodate the increase in arterial flow to the extremity, and high venous pressure develops. The veins become engorged and tense, which causes a bursting sensation or pain that is slowly relieved by rest. The same symptoms can be seen in individuals with chronic venous insufficiency, where persistent venous thrombosis or valvular insufficiency can cause an increase in ambulatory venous pressure that results in chronic lower extremity edema and evidence of postphlebitic skin changes. In these patients, swelling is frequently minimal in the morning but progresses throughout the day with increased activity and dependency of the extremity.
Other Considerations in Young Patients.
Claudication of a vascular etiology most commonly occurs in patients 50 years or older. In younger patients, symptoms of effort discomfort can be associated with popliteal artery obstruction from muscular or tendinous entrapment or mucinous degeneration of the artery. Popliteal artery entrapment11 and popliteal adventitial cystic disease are uncommon conditions usually seen in patients younger than 50 years old (see Chapter 115). Another condition that can be seen in younger patients is chronic compartment syndrome, an overuse syndrome that is often symmetric and bilateral12,13 (see Chapter 163). The most common complaints are muscle cramping and swelling, with focal paresthesias on the plantar or dorsal aspect of the foot. The pain or discomfort is associated with tightness in the calf and is precipitated by exercise. The patient is often an athlete or a runner with large calf muscles. Muscle swelling, increased compartment pressure, and impaired venous outflow constitute a vicious circle. The pain usually starts after considerable exercise and does not quickly subside with rest.
Pain at Rest
Progressive, frequently multilevel atherosclerotic obstructive disease results in ischemic pain at rest. In the absence of acute embolic or thrombotic arterial occlusion, the onset of symptoms is gradual. In most cases, the patient will have a history of claudication. With injury or minor trauma, the patient may have associated nonhealing ulcers. Pain at rest represents a significant decrease in circulation and involves the most distal aspect of the lower extremity that is farthest from the central source of circulation and blood flow. The forefoot and digits are most commonly involved. In the absence of acute arterial occlusion, patients do not have pain in the thigh or calf at rest. The symptoms are classically relieved with dependency, because gravity tends to facilitate circulation. The symptoms are aggravated if the patient lies down and elevates the extremity, which further increases the work of pushing blood against gravity to the foot. Patients will complain that the pain awakens them at night or develops soon after lying down. It is not uncommon for patients to be unable to describe the character of the pain.
It is easiest to quantify the severity of pain at rest relative to the sleep that patients are able to obtain. Early in the course, patients may awaken only occasionally and are able to get back to sleep after sitting up or walking about the room. With time, patients may sleep with their foot constantly hanging over the edge of the bed. Eventually, it is necessary to sleep in a chair with the foot dependent. In the final stages, patients obtain little, if any, sleep.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


