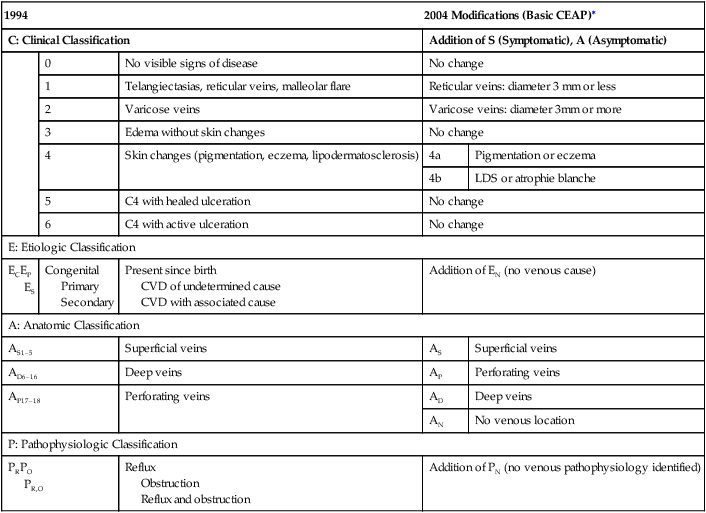
The clinical features of CVD involve a combination of historical, physical, and diagnostic findings. The CEAP classification system was proposed and initially adopted in 1994 in a consensus document. The CEAP clinical (C) classification is assigned during routine physical examination. The E, A, and P classifications serve to define the presence and nature of venous disease and to differentiate nonvenous causes that have similar physical findings (Table 1). However, assignment of clinical class was inconsistent, and the E, A, and P portions were considered cumbersome and difficult to use, and thus the original classification system was underutilized. Accordingly, the classification was revised in 2004 to better define the clinical classifications and to provide a more user-friendly version. TABLE 1 CVD, Chronic venous disease; LDS, lipodermatosclerosis.
Pathology and Classification of Chronic Venous Disease
In Search of Complete and Accurate Diagnosis
1994
2004 Modifications (Basic CEAP)∗
C: Clinical Classification
Addition of S (Symptomatic), A (Asymptomatic)
0
No visible signs of disease
No change
1
Telangiectasias, reticular veins, malleolar flare
Reticular veins: diameter 3 mm or less
2
Varicose veins
Varicose veins: diameter 3mm or more
3
Edema without skin changes
No change
4
Skin changes (pigmentation, eczema, lipodermatosclerosis)
4a
Pigmentation or eczema
4b
LDS or atrophie blanche
5
C4 with healed ulceration
No change
6
C4 with active ulceration
No change
E: Etiologic Classification
ECEP
ES
Congenital
Primary
Secondary
Present since birth
CVD of undetermined cause
CVD with associated cause
Addition of EN (no venous cause)
A: Anatomic Classification
AS1–5
Superficial veins
AS
Superficial veins
AD6–16
Deep veins
AP
Perforating veins
AP17–18
Perforating veins
AD
Deep veins
AN
No venous location
P: Pathophysiologic Classification
PRPO
PR,O
Reflux
Obstruction
Reflux and obstruction
Addition of PN (no venous pathophysiology identified)
Skin Pathology and Clinical Classification
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
