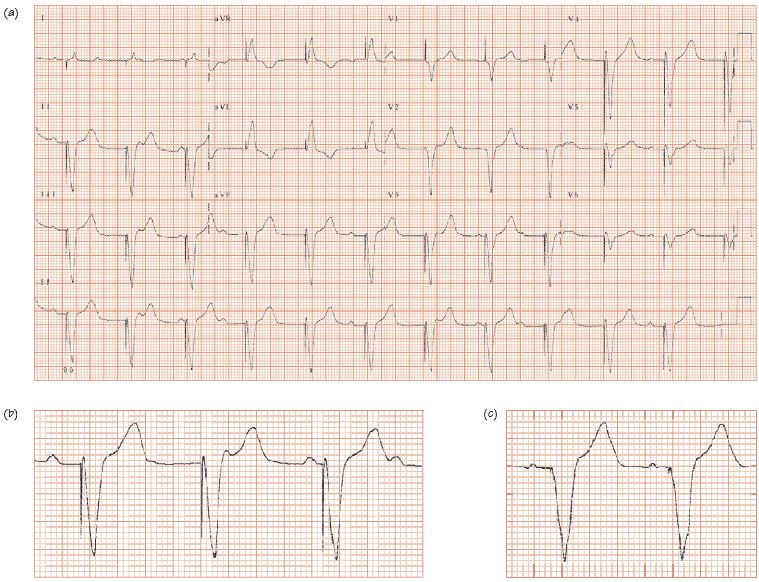
Fig. 58.2 (a) Paced ECG, VVI pacemaker. P waves occur randomly (examine the rhythm strip), unrelated to the QRS complexes. Pacing spike before each QRS complex, followed by a broad complex beat (electricity transmission from the electrode through the heart is by the slow myocyte-to-myocyte transmission). The QRS complexes for the standard ventricular pacemaker have a left bundle morphology (best shown in lead aVL), indicating the left ventricle is activated last, as the electrode is situated in the right ventricle. (b) Unipolar electrode – large pacing spike. (c) Bipolar electrode, small pacing spike.
Principle of pacing
Pacemakers treat slow heart rhythms (anti-bradycardia devices), fast heart rhythms (anti-tachycardia devices) and improve ventricular function in heart failure (cardiac resynchronization therapy [CRT]). These functions can be combined. Pacemakers work because:
- Cardiac activity is associated with current flow, which can be detected.
- An intrinsic property of the heart is that an action potential firing in a few cells spreads as a self-propagating wave throughout that chamber. Pacemakers listen out for normal heart activity, and if this does not occur, induce action potentials by passing depolarizing currents into a cardiac chamber (1–5 V, for 1–2 ms) triggering a self-propagating wave so restoring chamber electrical and thus mechanical function.
Pacemaker components
- An electrode(s) to pass electricity from spontaneous cardiac activity into the generator, and electricity from the pacemaker into the heart (Fig. 58.1).
- A generator

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


