The comparative operative mortality (OM) in women and men undergoing isolated coronary artery bypass graft surgery (CABG) has not been clarified. Therefore, we evaluated factors related to OM in a large cohort of women and men undergoing isolated CABG. Results from 121 hospitals on patients undergoing isolated CABG in 2003 and 2004 were analyzed according to gender, including demographics, clinical characteristics, and surgical outcome. A total of 10,708 women and 29,669 men had isolated CABG in 2003 to 2004. Observed mortality in women was significantly higher than in men (4.60% vs 2.53%, p <0.0001). Although men had a higher prevalence of >3 diseased coronary arteries and left ventricular dysfunction, women were more likely to be older, diabetic, have stage 3 to 5 chronic kidney disease, chronic lung disease, and nonelective CABG. Women were less likely to receive an internal mammary artery graft. Multivariate analysis indicated that women were at higher risk for OM than men (odds ratio 1.61, 95% confidence interval 1.40 to 1.84). In conclusion, data from the large state-mandated CCORP indicate that women are at increased risk of OM after isolated CABG compared to men, despite adjustment for preoperative risk factors.
Most studies on coronary artery bypass graft surgery (CABG) have reported that operative mortality (OM) with this procedure is higher in women than in men. Despite the decrease in overall OM in patients undergoing CABG over the previous decade, this difference has persisted. However, a recent propensity analysis found no effect of gender on OM with CABG, but excluded 74% of women in the cohort because they could not be matched, limiting generalizability of these results. Due to the need for improved understanding of factors associated with OM in women undergoing CABG, we evaluated data on gender and OM in the 2003 and 2004 California CABG Outcomes Reporting Program (CCORP).
Methods
All hospitals in the state of California licensed to perform CABG are required to report all isolated CABGs to the CCORP, under a state mandate. Data collection includes a rigorous system of audit including risk-adjusted OM. Isolated CABG is defined as CABG performed without other major cardiac procedures during the same operation. Detailed description of the CCORP data collection and analysis methodology has been previously described, including the 25 specific factors used in our multivariable risk models.
Data from 121 hospitals in which isolated CABG was performed during 2003 and 2004 were analyzed, including patient demographics, clinical characteristics, and observed OM. Gender was the primary independent variable and the primary study outcome was OM. The CCORP clinical data registry used a subset of 25 data elements collected by the Society of Thoracic Surgeons (STS) for their National Database of Cardiac Surgery. “Salvage” surgery was used to denote CABG that was performed in a patient undergoing cardiopulmonary resuscitation en route to the operating room or before anesthesia induction. Emergency surgery was defined as CABG performed in a patient with any of the following: acute ischemic dysfunction despite maximal medical therapy (medical and/or intra-aortic balloon pump), evolving myocardial infarction, pulmonary edema requiring intubation, or cardiogenic shock. Renal function was classified according to chronic renal disease stages as recommended by the National Kidney Foundation.
OM was defined as death occurring in hospital after CABG, regardless of length of stay or death occurring anywhere after hospital discharge within 30 days of CABG. However, in contrast to STS, to ensure accurate capture of deaths, the CCORP data were linked to vital statistics information from the California Department of Health Services to identify patients who died at home or at facilities other than the operating hospital within 30 days after CABG.
Statistical analysis
We used descriptive statistics to compare demographic and clinical variables. General linear model for analysis of variance and CONTRST were applied to identify significant differences in baseline characteristics, clinical presentation, and CABG details between men and women. Continuous variables are presented as mean ± SD. A p value <0.05 was considered statistically significant. We used the method of recycled predictions to determine the effect of gender on OM after controlling for demographic and clinical risk factors. This method is necessary because the multivariable logistic regression model is nonlinear; the predicted marginals allowed us to compare patients of different genders as if they had, on average, the same attributes for all other model covariates. Using the estimated coefficients from the risk model, we estimated the probabilities of OM if all patients were assumed to be men and then if all patients were assumed to be women. The difference between these 2 average predicted OM rates reflects the net effect of gender on OM, controlling for all other risk factors. All data analyses were conducted using SAS 9.1.3 (SAS Institute, Cary, North Carolina).
Results
In 2003 to 2004, 40,377 patients with isolated CABG were reported to the CCORP database, including 10,708 women and 29,669 men. Their baseline characteristics are listed in Table 1 . Women tended to be older than men, had a higher prevalence of diabetes, stage ≥3 renal dysfunction, and more chronic lung disease and hypertension. More women compared to men were referred for urgent CABG, had heart failure, and had moderate to severe mitral regurgitation. Women were significantly less likely to receive internal mammary artery grafts. Men had a higher prevalence of left ventricular (LV) dysfunction (LV ejection fraction <40%), larger number of diseased coronary vessels, and higher prevalence of previous CABG.
| Variable | Men | Women | p Value |
|---|---|---|---|
| (n = 29,669) | (n = 10,708) | ||
| Age (years) | |||
| <65 | 45.53% | 33.46% | <0.0001 |
| 65–74 | 32.06% | 34.40% | |
| >75 | 22.41% | 32.13% | |
| Race | |||
| Caucasian | 71.28% | 66.32% | <0.0001 |
| African-American | 11.49% | 13.88% | <0.0001 |
| Hispanic | 2.97% | 5.66% | <0.0001 |
| Asian | 8.78% | 8.93% | 0.652 |
| Body mass index (kg/m 2 ) | |||
| <18.5 | 0.62% | 1.79% | <0.0001 |
| 18.5–39.9 | 96.74% | 92.59% | |
| >40 | 2.64% | 5.61% | |
| Acuity | |||
| Elective | 37.29% | 31.29% | <0.0001 |
| Urgent | 57.26% | 62.26% | <0.0001 |
| Emergency | 5.27% | 6.12% | 0.001 |
| Salvage | 0.18% | 0.33% | 0.0061 |
| Diabetes mellitus | 35.88% | 46.82% | <0.0001 |
| Chronic kidney disease | |||
| Stage 1–2 | 76.54% | 57.56% | <0.0001 |
| Stage 3 | 19.68% | 35.15% | |
| Stage 4 | 1.25% | 3.48% | |
| Stage 5 | 2.53% | 3.81% | |
| Hypertension | 76.51% | 85.14% | <0.0001 |
| Chronic lung disease | 17.15% | 18.55% | 0.001 |
| Heart failure | 16.11% | 22.25% | <0.0001 |
| Left main coronary artery stenosis (>50%) | 25.01% | 25.10% | 0.8537 |
| Left ventricular ejection fraction <40% | 19.34% | 16.47% | <0.0001 |
| ≥3 narrowed coronary arteries | 79.87% | 73.59% | <0.0001 |
| Mitral regurgitation, moderate/severe | 2.90% | 5.20% | <0.0001 |
| Previous coronary artery bypass graft surgery | 5.91% | 4.23% | <0.0001 |
| Internal mammary artery use | |||
| Left and/or right | 89.25% | 83.55% | <0.0001 |
| Left only | 85.12% | 81.23% | <0.0001 |
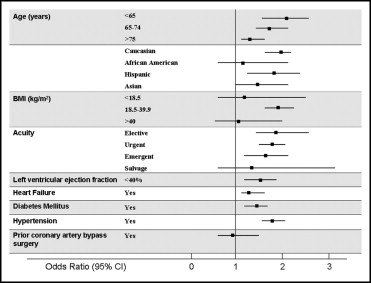
Observed OM in women was significantly higher than in men (4.60% vs 2.53%, p <0.0001). On multivariate analysis, women had a significantly higher risk of OM (odds ratio [OR] 1.61, 95% confidence interval [CI] 1.41 to 1.84). When the method of recycled predictions was applied, female gender remained a significant predictor of risk adjusted OM (p <0.0001). As shown in Figure 1 , women across all age groups had a higher OM compared to men. Women with diabetes, hypertension, heart failure, chronic lung disease, and LV dysfunction had a significantly higher OM. Younger women compared to younger men (<65 years of age) had the highest OR for OM (OR 2.31), as did women with left main coronary artery disease and 3-vessel disease (OR 1.91). There were no significant differences in outcomes between men and women who underwent salvage surgery or who had previous CABG. OM was higher in women with body mass index 18 to 39.9 kg/m 2 compared to men (OR 1.89, 95% CI 1.68 to 2.13, p <0.0001). This difference was not seen in women compared to men with body mass index <18 or >39.9 kg/m 2 .