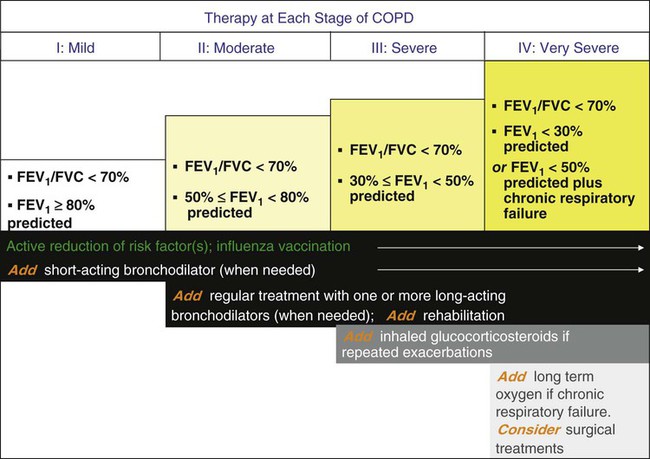
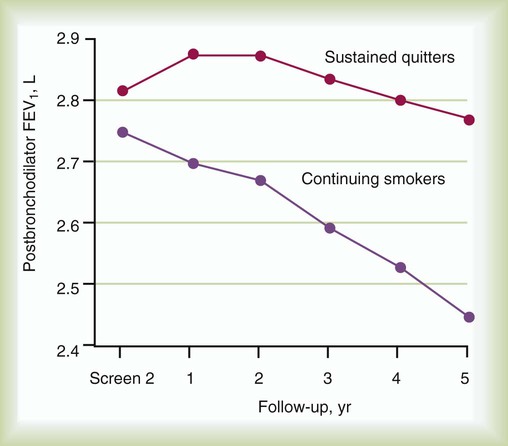
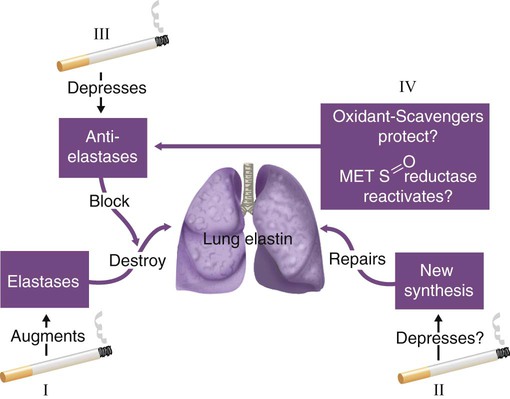
After reading this chapter you will be able to: The term chronic obstructive pulmonary disease (COPD), or sometimes chronic obstructive lung disease (COLD), refers to a disease state characterized by the presence of incompletely reversible airflow obstruction. New guidelines by the American Thoracic Society (ATS) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend the use of the term COPD to encompass both chronic bronchitis and emphysema. The ATS guidelines statement regarding COPD define this entity as follows1: Similarly, the GOLD guidelines define COPD as “a disease state characterized by airflow limitation that is not fully reversible, is usually progressive, and is associated with an abnormal inflammatory response of the lungs to noxious particles or gases.”2 The spectrum of COPD is shown in Figure 23-1, which presents a nonproportional Venn diagram representing the major components of COPD—chronic bronchitis and emphysema. Although asthma is no longer conventionally considered to be part of the spectrum of COPD, the diagram shows that considerable overlap between asthma and COPD exists. In actual practice, individuals with a history of asthma but with incompletely reversible airflow obstruction may be indistinguishable from patients with COPD. The two major entities constituting COPD—emphysema and chronic bronchitis—are defined in different ways. Emphysema is defined in anatomic terms as a condition characterized by abnormal, permanent enlargement of the airspaces beyond the terminal bronchiole, accompanied by destruction of the walls of the airspaces without fibrosis. Chronic bronchitis is defined in clinical terms as a condition in which chronic productive cough is present for at least 3 months per year for at least 2 consecutive years. The definition specifies further that other causes of chronic cough (e.g., gastroesophageal reflux, asthma, and postnasal drip) have been excluded. Figure 23-1 shows considerable overlap between chronic bronchitis and emphysema and some overlap with asthma—that is, when airflow obstruction is incompletely reversible. Figure 23-1 also shows that chronic bronchitis and emphysema can occur without airflow obstruction, although the clinical significance of these diseases usually stems from obstruction to airflow. COPD is one of the most frequent causes of morbidity and mortality worldwide.3 The World Health Organization predicts that COPD will become the fifth most prevalent disease in the world and the fourth leading cause of worldwide mortality by 2020. In the United States, COPD is currently the third leading cause of death; it was responsible for 145,075 deaths in 2008.4 Estimates suggest that 24 million Americans are affected.4–6 Data from the National Health and Nutrition Examination Survey (NHANES) suggest that among adults 25 to 75 years old in the United States, mild COPD (defined as forced expiratory volume in 1 second [FEV1]/forced vital capacity [FVC] <70%, and FEV1 >80% predicted) occurs in 6.9% and moderate COPD (defined as FEV1/FVC <79% and FEV1 ≤80% predicted) occurs in 6.6%.3 COPD prevalence increases with aging, with a fivefold increased risk for adults older than 65 years compared with adults younger than 40 years, and some studies estimate a prevalence of 20% to 30% in adults older than 70 years.7 The growing health burden from COPD is caused in part by the aging of the population but mainly by the continued use of tobacco. The socioeconomic burden of COPD is also substantial. In 2000, COPD caused 726,000 hospitalizations (which accounted for 1.9% of all hospitalizations in the United States), 7,997,000 office visits to physicians, and 1,549,000 emergency department visits, and, in 2002, COPD resulted in a total health expenditure of $32.1 billion.3 In this regard, COPD is a problem that is a frequent challenge for the respiratory clinician. Although many risk factors exist for COPD (Box 23-1), the two most common are cigarette smoking (which has been estimated to account for 80% to 90% of all COPD-related deaths) and alpha1-antitrypsin (AAT) deficiency.8 Evidence linking cigarette smoking to the development of COPD is strong and includes the following: • Symptoms of COPD (e.g., chronic cough and phlegm production) are more common in smokers than in nonsmokers. • Impaired lung function with evidence of an obstructive pattern of lung dysfunction is more common in smokers than in nonsmokers. • Pathologic changes of airflow obstruction and chronic bronchitis are evident in the lungs of smokers. • So-called susceptible smokers, who represent approximately 15% of all cigarette smokers, experience more rapid rates of decline of lung function than nonsmokers. Information from the Lung Health Study (Figure 23-2) highlighted the accelerated rate of decrease of FEV1 in smokers compared with former smokers who have achieved sustained quitting.9,10 Overall, the strength of evidence implicating cigarette smoking as a cause of COPD has allowed the U.S. Surgeon General to conclude, “Cigarette smoking is the major cause of chronic obstructive lung disease in the United States for both men and women. The contribution of cigarette smoking to chronic obstructive lung disease morbidity and mortality far outweighs all other factors.”11 As the second well-recognized cause of emphysema, AAT deficiency, sometimes called genetic emphysema, is a condition characterized by a deficient amount of the protein AAT, which may result in the early onset of emphysema and which is inherited as a so-called autosomal codominant condition. Accounting for 2% to 3% of all cases of COPD, AAT deficiency is severely underrecognized by health care providers but affects an estimated 100,000 Americans. In one 1995 survey, the mean interval between the first onset of pulmonary symptoms and initial diagnosis of AAT deficiency was 7.2 years, and 43% of individuals with severe deficiency of AAT reported seeing at least three physicians before the diagnosis of AAT deficiency was first made.12 More recent studies suggested that underrecognition of AAT deficiency persisted as of 2003 and that the diagnostic delay interval had not decreased significantly.12–14 The importance of early identification is emphasized by the need to test (by simply sending a serum level for AAT) first-degree relatives (e.g., siblings, parents, and children), by the favorable effect of primary prevention of smoking among individuals identified early, and by the availability of a specific therapy called intravenous augmentation therapy. The risk of developing emphysema for individuals with AAT deficiency increases as the serum AAT level decreases to less than 11 µmol/L, or less than approximately 57 mg/dl using nephelometry, and is enhanced by cigarette smoking.14 Study of AAT deficiency has helped formulate the protease-antiprotease hypothesis of emphysema.14,15 In this explanatory model (Figure 23-3), lung elastin, a major structural protein that supports the alveolar walls of the lung, is normally protected by AAT, a protein that opposes the degradative threat of neutrophil elastase. Neutrophil elastase is a protein contained within neutrophils that is released when neutrophils are attracted to the lung during inflammation or infection. Under normal circumstances of an adequate amount of AAT, neutrophil elastase is counteracted so as not to digest lung elastin. However, in the face of a severe deficiency of AAT (i.e., when serum levels decrease below a “protective threshold” value of 11 µmol/L, or 57 mg/dl), neutrophil elastase may go unchecked, causing breakdown of elastin and resulting in dissolution of alveolar walls. This protease-antiprotease model explains the pathogenesis of emphysema in AAT deficiency, but evidence suggesting its role in COPD in individuals with normal amounts of AAT is conflicting. Also, other proteases (e.g., matrix metalloproteinases and inflammation) are thought to contribute to the proteolysis that produces emphysema.16 COPD may occur in the absence of active cigarette smoking or AAT deficiency (see Box 23-1).17,18 Factors such as passive smoking, air pollution, occupational exposure, and airway hyperresponsiveness may contribute to fixed airflow obstruction. The mechanisms of airflow obstruction in COPD include inflammation and obstruction of small airways (<2 mm in diameter); loss of elasticity, which keeps small airways open when elastin is destroyed in emphysema; and active bronchospasm. Although traditionally considered to be characteristic of asthma, some reversibility of airflow obstruction has been observed in up to two-thirds of COPD patients when tested serially with inhaled bronchodilators.19 Common symptoms of COPD include cough, phlegm production, wheezing, and shortness of breath, typically on exertion. Dyspnea is often slow but progressive in onset and occurs later in the course of the disease, characteristically in the late sixth or seventh decade of life. One notable exception is AAT deficiency, in which dyspnea characteristically begins sooner (mean age approximately 45 years).8 Table 23-1 reviews the characteristic features of emphysema and chronic bronchitis and emphasizes traits that should suggest the possibility of AAT deficiency, including early onset of emphysema, emphysema in a nonsmoker, or a family history of emphysema. Suspicion of AAT deficiency should lead to a simple blood test by which the serum level can be established.8,14 TABLE 23-1 In managing patients with chronic, stable COPD, the following goals must guide the clinician1,2: • Establish the diagnosis of COPD. • Maximize the patient’s functional status. • Simplify the medical regimen as much as possible. In managing an acute exacerbation of COPD, additional considerations are to reestablish the patient to baseline status as quickly and with as little incidence of morbidity and mortality as possible.20,21 Each of the treatments discussed in this section is considered in the context of these goals, recognizing differences in management between patients with chronic, stable COPD versus an acute exacerbation of COPD. In patients with COPD, PaCO2 usually is generally preserved until airflow obstruction is severe (FEV1 < 1 L), when the PaCO2 level may increase. After the diagnosis of COPD is established, a secondary issue is for the clinician to consider whether the patient has an underlying predisposition to COPD, such as AAT deficiency or other cause listed in Box 23-1.17,18 Underlying causes are present in fewer than 5% of patients with COPD, with AAT deficiency being the most common (2% to 3% of all patients with COPD). Mini Clini Determining the Severity of Chronic Obstructive Pulmonary Disease The severity of COPD is described by the degree of airflow obstruction. Traditional descriptors such as hypoxemia and hypercapnia are useful for characterizing COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has proposed a staging system for COPD.2 According to this staging system, patients are categorized into one of the following four stages: Although airflow obstruction from emphysema itself is irreversible, most (up to two-thirds) patients with stable COPD exhibit a reversible component of airflow obstruction, defined as a 12% and 200-ml increase in postbronchodilator FEV1 or FVC or both. For this reason, as indicated in an algorithm developed by GOLD (Figure 23-4),2,22–24 bronchodilator therapy is recommended for patients with COPD. Bronchodilators produce smooth muscle relaxation resulting in improved airflow obstruction, improved symptoms and exercise tolerance, and decrease in the frequency and severity of exacerbations, but they do not enhance survival. The results of the Lung Health Study,9 which compared the effects of inhaled ipratropium bromide (two puffs four times daily) with placebo in patients with mild, stable COPD, showed that regular, long-term use of ipratropium did not change the rate of decline of lung function but offered a one-time, small increase in FEV1. Both anticholinergic and adrenergic (beta agonist) bronchodilators can improve airflow in patients with COPD, although some clinicians favor an inhaled anticholinergic medication (e.g., ipratropium bromide or tiotropium22–24) as first-line therapy (Figure 23-5). More recent concerns about the possible adverse cardiovascular effects of anticholinergic therapy in patients with COPD25 have been dismissed by the results of a multicenter trial (UPLIFT [Understanding Potential Long-Term Impacts on Function with Tiotropium]), which found a significantly lower rate of cardiac adverse events and cardiovascular death in patients who received tiotropium.26 The GOLD guidelines2 recommend the use of short-acting beta-adrenergic agents (≤6 hours) for symptomatic management of all patients with COPD. Also, the use of a long-acting beta agonist (e.g., salmeterol) or a long-acting anticholinergic drug (e.g., tiotropium) can lessen the frequency of acute exacerbations of COPD.25 Other treatment options to optimize lung function include administering corticosteroids and methylxanthines. Systemic corticosteroids can produce significant improvements in airflow in a few (6% to 29%) patients with stable COPD.27 To assess whether airflow obstruction is completely reversible (i.e., the patient has asthma) and whether a patient with COPD is responsive to steroids, a brief course of corticosteroids (20 to 40 mg/day of prednisone or equivalent for 10 to 14 days) is often recommended. Patients with a significant clinical response often are treated with long-term inhaled corticosteroids or rarely with the smallest necessary dose of systemic corticosteroids, recognizing that long-term systemic steroid therapy has risks.28 Also, results of several major clinical trials (e.g., Lung Health Study II, Euroscop, ISOLDE, and Copenhagen City Study but not TORCH) agree that inhaled corticosteroids do not change the rate of decline of FEV1 in patients with COPD, although their use is associated with a decreased frequency of acute exacerbations.29,30 Studies of combined salmeterol and fluticasone versus placebo in patients with COPD suggest that adding an inhaled corticosteroid (fluticasone) to the long-acting beta agonist (salmeterol) can improve FEV1 and can reduce the frequency of acute exacerbations of COPD but does not improve survival.29,30 The finding of a higher rate of pneumonia in inhaled corticosteroid users is concerning. Overall, the GOLD guidelines2 recommend use of inhaled corticosteroids in patients with FEV1 less than 50% and history of recurrent exacerbations (three episodes in the last 3 years), whereas the ATS/European Respiratory Society (ERS) guidelines recommend use of inhaled corticosteroids in patients with FEV1 less than 50% who have required use of oral corticosteroids or oral antibiotics at least once within the last year.31 Treatment with methylxanthines offers little additional bronchodilation in patients using inhaled bronchodilators and generally is reserved for patients with debilitating symptoms from stable COPD despite optimal inhaled bronchodilator therapy. Controlled trials show lessened dyspnea in methylxanthine recipients despite a lack of measurable increases in airflow.32 Side effects of methylxanthines include anxiety, tremulousness, nausea, cardiac arrhythmias, and seizures. To minimize the chance of toxicity, current recommendations suggest maintaining serum theophylline levels at 8 to 10 mcg/ml. Strategies for improving lung function during acute exacerbations of COPD generally include inhaled bronchodilators (especially beta-2 agonists), antibiotics, and systemic corticosteroids. Because of their rapid onset of action and efficacy, short-acting beta-2 agonists are first-line therapy for patients with COPD exacerbation. Inhaled beta-2 agonists are frequently administered through a nebulizer, although metered dose inhaler devices may have equal efficacy if administered appropriately.2 A common practice is to administer 2.5 mg of albuterol by nebulizer every 1 to 4 hours as needed. Higher doses of albuterol (i.e., 5 mg) do not produce further improvement in pulmonary function and may cause cardiac side effects.33 Similarly, continuous nebulization of short-acting beta-2 agonists in patients with COPD exacerbation is not recommended. In addition to inhaled bronchodilator therapy, short-term systemic corticosteroids are recommended to reduce inflammation and improve lung function. An early randomized, controlled trial of intravenous methylprednisolone for patients with acute exacerbations showed accelerated improvement in FEV1 within 72 hours.34 Larger, more recent trials have confirmed the benefits of systemic corticosteroids in acute exacerbations and have shown that short-term oral courses (i.e., approximately 2 weeks) are as effective as longer courses (i.e., 8 weeks) with fewer adverse steroid effects.35 For patients with acute exacerbations characterized by purulent phlegm, oral antibiotics (e.g., trimethoprim-sulfamethoxazole, amoxicillin, or doxycycline) administered for 7 to 10 days have produced accelerated improvement of peak flow rates compared with placebo recipients.20,36,37 Finally, intravenous methylxanthines offer little benefit in the setting of acute exacerbations of COPD and have fallen into disfavor.38,39 Taken together, important elements of managing an acute exacerbation of COPD caused by purulent bronchitis include supplemental oxygen (O2) to maintain arterial saturation at greater than 90%, inhaled bronchodilators, oral antibiotics, and a brief course of systemic corticosteroids.20 For patients with hypercapnia and acute respiratory acidemia, the clinician also must decide whether to institute ventilatory assistance. Although intubation and mechanical ventilation historically have been the preferred approach, more recent studies suggest that noninvasive positive pressure ventilation can be an appealing alternative for patients with acute exacerbations of COPD, especially with severe exacerbations characterized by pH less than 7.30.40 Specifically, based on available randomized, controlled clinical trials showing that noninvasive positive pressure ventilation can shorten intensive care unit (ICU) stay and avert the need for intubation, the American Association for Respiratory Care consensus conference and guidelines on noninvasive ventilation from other official societies have endorsed this approach.41,42 Criteria defining candidacy for noninvasive ventilation include acute respiratory acidosis (without frank respiratory arrest); hemodynamic stability; ability to tolerate the interface needed for noninvasive ventilation; ability to protect the airway; and lack of craniofacial trauma or burns, copious secretions, or massive obesity.41 In symptomatic patients with stable COPD, maximizing their ability to perform daily activities is a priority (see Figure 23-4). Pharmacologic treatments to maximize functional status include administration of bronchodilators to enhance lung function as much as possible and consideration of methylxanthine therapy, based on data that such drugs can lessen dyspnea and improve functional status ratings even in the absence of improved airflow.32 Comprehensive pulmonary rehabilitation is a multidisciplinary intervention that consists of lower and upper extremity exercise conditioning, breathing retraining, education, and psychosocial support. Pulmonary rehabilitation is an additional important strategy for improving functional status.43 Randomized, controlled trials show that although pulmonary rehabilitation does not improve lung function or survival, this strategy results in decreased dyspnea perception, improved health-related quality of life, fewer days of hospitalization, and decreased health care usage.44,45 Finally, transcutaneous neuromuscular electrical stimulation is a new experimental therapy that has been successfully used to stimulate peripheral muscles in patients with COPD. Studies have shown significant improvements in quadriceps muscle function, exercise tolerance (including walk distance), and health status in patients with severe COPD.46 Follow-up data from the Lung Health Study9 confirm that a comprehensive smoking cessation program (including instruction, group counseling, and nicotine replacement therapy) can achieve sustained smoking cessation in 22% of participants and that the rate of annual FEV1 decline in these sustained nonsmokers was significantly less than it was for continuing smokers, even over 11 years of follow-up.10 Participation in aggressive smoking cessation can enhance survival rates in patients with COPD.10 Critical elements in achieving successful abstinence from smoking include identifying “teachable moments” (i.e., during episodes of illness where smoking can be identified as a contributing factor47), identifying the role of smoking in adverse health outcomes, negotiating a “quit date,” and providing frequent follow-up reminders from health care providers.48 A helpful strategy during counseling is to use the five A’s of smoking cessation2: In this regard, the respiratory therapist (RT), who sees the patient frequently, has a special responsibility to provide frequent, constructive reminders about the advisability of smoking cessation.49 Among available treatments for COPD, supplemental oxygen is important because, similar to smoking cessation and lung volume reduction surgery in selected individuals (see later), it can prolong survival.50–53 Box 23-2 reviews the indications for supplemental O2, and Figure 23-5 shows the results of the American Nocturnal Oxygen Therapy Trial50 and the British Medical Research Council trial of domiciliary O2 (1980-1981).51,52
Obstructive Lung Disease
Chronic Obstructive Pulmonary Disease (COPD), Asthma, and Related Diseases
 State definitions of chronic obstructive pulmonary disease (COPD), asthma, and bronchiectasis.
State definitions of chronic obstructive pulmonary disease (COPD), asthma, and bronchiectasis.
 Identify how many Americans are diagnosed with COPD and how many deaths from COPD occur each year.
Identify how many Americans are diagnosed with COPD and how many deaths from COPD occur each year.
 Understand the major risk factors associated with the onset of COPD.
Understand the major risk factors associated with the onset of COPD.
 Identify the common signs and symptoms associated with COPD.
Identify the common signs and symptoms associated with COPD.
 State the factors associated with the onset of asthma.
State the factors associated with the onset of asthma.
 Describe the typical clinical presentation of a patient with asthma.
Describe the typical clinical presentation of a patient with asthma.
 Identify the treatment currently available for a patient with acute asthma.
Identify the treatment currently available for a patient with acute asthma.
 Describe the treatment currently available for patients with bronchiectasis.
Describe the treatment currently available for patients with bronchiectasis.
Chronic Obstructive Pulmonary Disease
Overview and Definitions
Epidemiology
Risk Factors and Pathophysiology
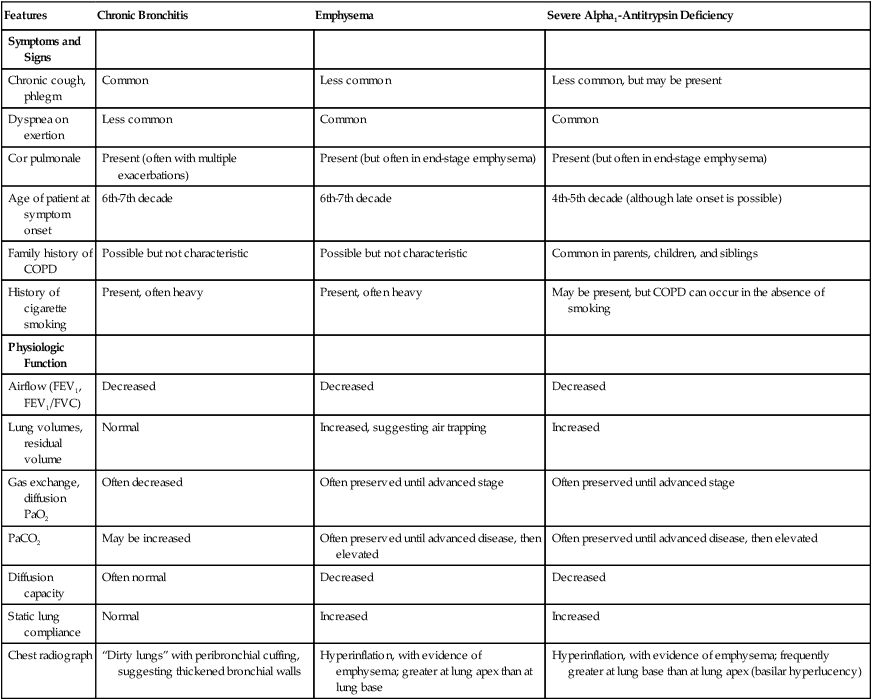
Clinical Signs and Symptoms
Features
Chronic Bronchitis
Emphysema
Severe Alpha1-Antitrypsin Deficiency
Symptoms and Signs
Chronic cough, phlegm
Common
Less common
Less common, but may be present
Dyspnea on exertion
Less common
Common
Common
Cor pulmonale
Present (often with multiple exacerbations)
Present (but often in end-stage emphysema)
Present (but often in end-stage emphysema)
Age of patient at symptom onset
6th-7th decade
6th-7th decade
4th-5th decade (although late onset is possible)
Family history of COPD
Possible but not characteristic
Possible but not characteristic
Common in parents, children, and siblings
History of cigarette smoking
Present, often heavy
Present, often heavy
May be present, but COPD can occur in the absence of smoking
Physiologic Function
Airflow (FEV1, FEV1/FVC)
Decreased
Decreased
Decreased
Lung volumes, residual volume
Normal
Increased, suggesting air trapping
Increased
Gas exchange, diffusion PaO2
Often decreased
Often preserved until advanced stage
Often preserved until advanced stage
PaCO2
May be increased
Often preserved until advanced disease, then elevated
Often preserved until advanced disease, then elevated
Diffusion capacity
Often normal
Decreased
Decreased
Static lung compliance
Normal
Increased
Increased
Chest radiograph
“Dirty lungs” with peribronchial cuffing, suggesting thickened bronchial walls
Hyperinflation, with evidence of emphysema; greater at lung apex than at lung base
Hyperinflation, with evidence of emphysema; frequently greater at lung base than at lung apex (basilar hyperlucency)
Management
Establishing the Diagnosis
Stage
Description
I
Patients with FEV1/FVC < 70% and FEV1 > 80% predicted
II
Patients with FEV1/FVC < 70% and FEV1 50%-79% predicted
III
Patients with FEV1/FVC < 70% and FEV1 30%-49% predicted
IV
Patients with FEV1/FVC < 70% and FEV1 < 30% or FEV1 < 50% predicted plus chronic respiratory failure
Optimizing Lung Function
Stable Chronic Obstructive Pulmonary Disease
Acute Exacerbations
Maximizing Functional Status
Preventing Progression of Chronic Obstructive Pulmonary Disease and Enhancing Survival
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Obstructive Lung Disease: Chronic Obstructive Pulmonary Disease (COPD), Asthma, and Related Diseases


 Rule Of Thumb
Rule Of Thumb Rule Of Thumb
Rule Of Thumb Problem
Problem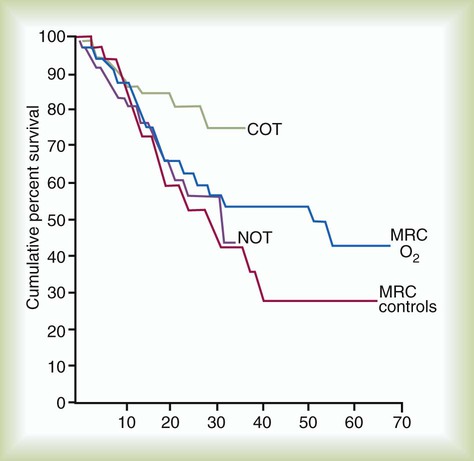
 Problem
Problem