Nomograms to predict normal aortic root diameter for body surface area (BSA) in broad ranges of age have been widely used but are limited by lack of consideration of gender effects, jumps in upper limits of aortic diameter among age strata, and data from older teenagers. Sinus of Valsalva diameter was measured by American Society of Echocardiography convention in normal-weight, nonhypertensive, nondiabetic subjects ≥15 years old without aortic valve disease from clinical or population-based samples. Analyses of covariance and linear regression with assessment of residuals identified determinants and developed predictive models for normal aortic root diameter. In 1,207 apparently normal subjects ≥15 years old (54% women), aortic root diameter was 2.1 to 4.3 cm. Aortic root diameter was strongly related to BSA and height (r = 0.48 for the 2 comparisons), age (r = 0.36), and male gender (+2.7 mm adjusted for BSA and age, p <0.001 for all comparisons). Multivariable equations using age, gender, and BSA or height predicted aortic diameter strongly (R = 0.674 for the 2 comparisons, p <0.001) with minimal relation of residuals to age or body size: for BSA 2.423 + (age [years] × 0.009) + (BSA [square meters] × 0.461) − (gender [1 = man, 2 = woman] × 0.267), SEE 0.261 cm; for height 1.519 + (age [years] × 0.010) + (height [centimeters] × 0.010) − (gender [1 = man, 2 = woman] × 0.247), SEE 0.215 cm. In conclusion, aortic root diameter is larger in men and increases with body size and age. Regression models incorporating body size, age, and gender are applicable to adolescents and adults without limitations of previous nomograms.
Aortic dilatation is strongly associated with presence and severity of aortic regurgitation and risk for aortic dissection. Nomograms to predict normal aortic root diameter for body surface area (BSA) in broad ranges of age have been widely used to detect aortic enlargement in clinical practice and adopted in guidelines. However, these nomograms were based on a modest-size reference population that did not permit definitive consideration of gender effects and are limited by jumps in upper limits of normal aortic diameter at transitions to older age strata and insufficient data on normal limits for older teenagers. In addition, it is uncertain whether use of BSA as the measurement of body size under-recognizes aortic dilatation in obese subjects. Accordingly, the present study assessed relations of aortic root diameter determined by echocardiography to age, gender, and height or BSA as alternative measurements of body size in a large population of apparently normal subjects ≥15 years old.
Methods
The present reference population included subjects who were nonobese, normotensive, nondiabetic, and free of clinically overt cardiovascular disease or aortic valve disease recognized by echocardiography from the following sources: (1) 143 subjects ≥15 years old from the New York population reported by Roman et al ; (2) 510 adolescents or adults who participated in the first examination of the Strong Heart Family Study cohort ; (3) 459 subjects ≥15 years old who underwent echocardiography in the second Family Blood Pressure Program examination ; and (4) 122 subjects ≥17 years old who had echocardiograms at the first or second Hypertension Genetic Epidemiology Network Study (HyperGEN) examination. Height and weight were measured by standardized methods at clinic examinations; BSA was calculated by the method of Dubois and Dubois : BSA (square meters) = 0.007184 × H 0.725 × W 0.425 , where H represents height in centimeters and W represents weight in kilograms.
This method has been shown to yield BSA values similar to those from the Haycock and other formulas in subjects with BSA >0.7 m 2 , encompassing the range of body sizes in the present study population. Because BSA is a second-power measurement and aortic diameter is a first-power measurement, BSA 0.5 was considered in alternative analyses.
Echocardiograms were recorded by standardized methods and centrally read at Cornell Medical Center. Parasternal long- and short-axis views were used to record on videotape ≥10 consecutive beats of 2-dimensional and M-mode recordings of the aortic root and left atrium and of left ventricular internal diameter and wall thicknesses at or just below the tip of the anterior mitral leaflet; color Doppler was used to search for mitral and aortic regurgitations. The apical window was used to record ≥10 cycles of 2-, 3-, 4-, and 5-chamber images and color Doppler recordings to assess left ventricular wall motion and identify mitral and aortic regurgitations. Subjects with bicuspid aortic valves or with more than mild aortic or mitral regurgitation or any degree of aortic stenosis were excluded from the present analyses.
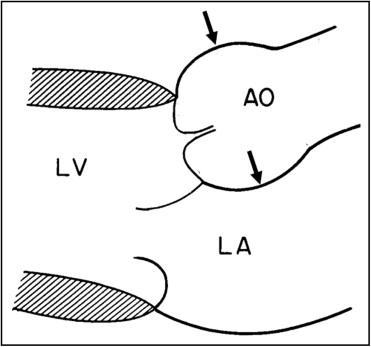
Echocardiograms were preliminarily read by a first reader and over-read by highly experienced readers (R.B.D. in >90%) blinded to subjects’ clinical data. Aortic root diameter was measured as previously described at end-diastole by the leading-edge convention in the parasternal or occasionally apical long-axis view that showed the maximum diameter parallel to the aortic annular plane ( Figure 1 ). Aortic annular diameter was measured between the hinging points of the right and noncoronary cusps of the aortic valve in systole.
Data are reported as mean ± SD for continuous variables or proportion for categorical variables. Univariate relations of continuous variables of age and measurements of body size with sinus of Valsalva diameters were assessed by least squares linear correlation. Differences between genders were assessed by t tests for independent samples in the entire population and in subgroups 15 to 24, 25 to 34, 35 to 44, 45 to 54, 55 to 64, and ≥65 years of age. Age, gender, and body size measurements were significantly related to aortic root diameter in univariate analyses; they were then entered in multiple linear regression models considering age, gender, and BSA or height as independent variables and sinus of Valsalva diameter as the dependent variable. Residuals of observed aortic diameter versus that predicted by multivariate models were calculated and their relations to age, primary measurements of body size (BSA or height), and body mass index were assessed. Two-tailed p value <0.05 was considered statistically significant.
Results
New York subjects included 70 women and 73 men 41 ± 16 years old (range 15 to 74) with mean BSA 1.83 ± 0.21 m 2 (1.29 to 2.40), height 1.67 ± 0.14 m (1.52 to 1.91), weight 68 ± 16 kg (49 to 110 kg), and aortic root diameter 3.13 ± 0.42 cm (2.1 to 4.3). Strong Heart Study participants included 288 American Indian women and 222 American Indian men 41 ± 16 years old (range 15 to 86) with mean BSA 1.71 ± 0.15 m 2 (1.27 to 2.32), height 1.68 ± 0.09 m (1.47 to 2.06), weight 62 ± 9 kg (38 to 97), and aortic root diameter 3.12 ± 0.31 cm (2.4 to 4.3). Family Blood Pressure Program participants included 240 women and 219 men 41 ± 14 years old (range 15 to 78) with mean BSA 1.71 ± 0.20 m 2 (1.25 to 2.41), height 1.67 ± 0.11 m (1.43 to 1.98), weight 63 ± 11 kg (35 to 108), and aortic root diameter 3.18 ± 0.39 cm (2.2 to 4.3); 166 were of African-American, 120 of Hispanic, and 173 of Japanese-American ethnicity. HyperGEN participants included 70 women and 52 men 33 ± 9 years old (range 17 to 50) with mean BSA 1.75 ± 0.19 m 2 (1.13 to 2.25), height 1.70 ± 0.10 m (1.49 to 1.92), weight 65 ± 11 kg (41 to 99), and aortic root diameter 3.08 ± 0.31 cm (2.4 to 3.9); 60 were of African-American and 62 of Caucasian ethnicity.
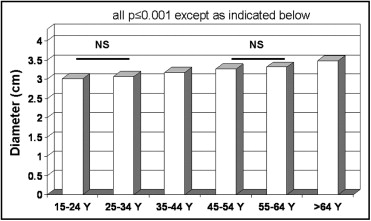
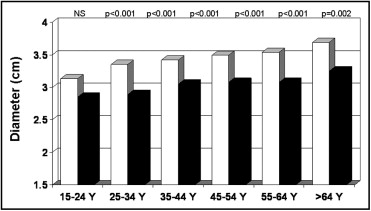
Aortic diameters at sinus of Valsalva showed highly significant positive univariate relations with age (r = 0.36), weight (r = 0.45), height (r = 0.14), BSA (r = 0.48), and BSA 0.5 (r = 0.48, p <0.001 for all comparisons). Age and each measurement of body size were independently related to sinus of Valsalva diameter in multiple linear regression models (p <0.001 for all comparisons). In analysis of covariance that adjusted for BSA, mean aortic diameter progressively increased at older ages (p <0.001; Figure 2 ) ; similar results were obtained using height as an alternative measurement for body size (data not shown). Men had larger mean aortic diameters than women in the entire population (3.34 ± 0.34 vs 2.98 cm, p <0.001). In analysis of covariance adjusted for BSA, aortic diameter tended to be larger in men than in women in the youngest age group (15 to 24 years old) and was significantly larger in men than in women in older age groups ( Figure 3 ). Multivariable models increased the coefficient of variation (r or R 2 ) for sinus of Valsalva diameter from 0.23 for BSA alone to 0.36 for BSA and age and to 0.45 when gender was also considered.
Multivariable models with age and gender yielded similar multiple R values (0.67 for the 2 comparisons) with BSA or height as the measurement of body size ( Table 1 ). SEEs, on which calculation of z scores is based, were 0.261 and 0.215 cm, respectively. Surfaces representing aortic diameters 1.96 z score above the predicted mean value of aortic diameter for age and BSA and for age and height are illustrated in Figure 4 for men and Figure 5 for women. There were no significant residual linear relations of age, gender, or body size measurements with the difference between observed sinus of Valsalva diameters and values predicted using BSA or height (p >0.20 for all comparisons). When absolute residuals were considered, only weak relations (r = 0.010 to 0.016) were observed. Multiple linear models that also considered body mass index did not improve on those using age, gender, and BSA (multiple R = 0.677 vs 0.674) or height (R = 0.679 vs 0.674, NS for the 2 comparisons).
| Variable | B | SE | Beta | t Test | p Value |
|---|---|---|---|---|---|
| Model with body surface area: dependent variable aortic root diameter (cm) | |||||
| Intercept | 2.423 | 0.261 | |||
| Age (decade) | 0.090 | 0.0044 | 0.387 | 20.3 | <0.0001 |
| Body surface area (m 2 ) | 0.461 | 0.036 | 0.467 | 21.7 | <0.0001 |
| Gender | |||||
| Male | −0.267 | 0.025 | −0.219 | −10.4 | <0.0001 |
| Female | −0.534 | ||||
| Model with body height: dependent variable aortic root diameter (cm) | |||||
| Intercept | 1.519 | 0.215 | |||
| Age (decade) | 0.10 | 0.004 | 0.429 | 25.2 | <0.0001 |
| Height (cm) | 0.010 | 0.001 | 0.387 | 14.8 | <0.0001 |
| Gender | |||||
| Male | −0.247 | 0.017 | −0.239 | −10.4 | <0.0001 |
| Female | −0.494 |
Aortic dilatation can be recognized when the difference between observed sinus of Valsalva diameter and the value predicted for age, gender, and body size >1.96 SEE (0.261 cm for model with BSA and 0.215 cm for model with height) above the predicted value. For convenience, mild, moderate, and severe aortic dilatation can be recognized by positive z score values from these models of 1.97 to 3.0, 3.01 to 4.0, and >4.0 according to a previously reported convention.
Multivariable models for aortic annular diameter had similar multiple R values (0.64 and 0.63, respectively) with age, gender, and BSA or height as the body size measurement ( Table 2 ). SEEs, on which calculation of z scores is based, were 0.113 and 0.070 cm, respectively. There were no significant residual linear relations of age, gender, or body size measurements with the difference between observed and predicted aortic annular diameters (p >0.20 for all comparisons). Only weak relations (r = 0.010 to 0.014) were observed for absolute residuals.



