Frequency-domain optical coherence tomography (FD-OCT) is becoming a useful diagnostic tool for coronary imaging for quantitative coronary analysis. Second-generation FD-OCT produces detailed coronary lumen images. However, the reproducibility of coronary measurements using FD-OCT in humans has not been thoroughly explored. Our goal was to determine the intraobserver, interobserver, and interpullback reproducibility of the in vivo FD-OCT measurements of the lumen area and/or lesion length. Twenty-five patients undergoing coronary angioplasty were included. In all subjects, FD-OCT pullbacks (20 mm/s) were acquired twice from the same coronary segment different from the target lesion, at an interval of 5 minutes, with no other intervention. A total of 9,396 cross-sectional lumen area frames and the relative coronary lesion length of each pullback were analyzed off-line with dedicated software by 2 independent expert readers (A and B). We compared the lumen area and length measurements as follows: pullback 1, read by reader A twice at an interval of 7 days (intraobserver analysis); pullback 1, independently read by readers A and B (interobserver comparison); and pullback 1 versus pullback 2, read by reader A (interpullback comparison). The per-segment and per-frame analyses showed very high and significant correlation coefficients for the interobserver, intraobserver, and interpullback comparisons for the lumen area and lesion length (R ≥0.95 and p <0.001 in all cases). Accordingly, the Bland-Altman estimates of bias showed nonsignificant differences in the interobserver, intraobserver, and interpullback comparisons at all levels, with average biases never >0.150 mm 2 for the lumen area or 0.200 mm for the lesion length. In conclusion, coronary imaging using FD-OCT showed excellent reproducibility, with low intraobserver, interobserver, and interpullback variability for both lumen area and lesion length measurements in humans. Thus, FD-OCT can be proposed for precise analysis in the catheterization laboratory to guide decision making and in clinical trials focusing on imaging end points.
Frequency-domain optical coherence tomography (FD-OCT) is an ultrahigh-resolution intracoronary imaging technology able to provide detailed images of the coronary lumen. Second-generation FD-OCT introduced significant improvements, simplifying data acquisition by increasing the speed of pullbacks, and significantly reducing patient discomfort. Thus, FD-OCT is rapidly being adopted by catheterization laboratories worldwide for clinical use and research purposes. This technique has great potential to become an instrumental tool to address lumen and plaque changes in response to specific pharmacologic or interventional treatment. Although intravascular ultrasonography has been frequently used for plaque progression/regression studies, FD-OCT, given its superior resolution, could become complementary or an alternative to intravascular ultrasonography in such research settings. However, limited data are available on the reproducibility of such data between separate pullbacks and between or within operators. In particular, the variability between and within operators and/or pullbacks has not been formally tested. We hypothesized that FD-OCT will allow reproducible measurements of the coronary lumen area and lesion length. Thus, we conducted a prospective study to systematically determine the reproducibility of FD-OCT measurements for the coronary lumen area and lesion length in humans.
Methods
The present study was a prospective single-center study approved by the local review board. Twenty-five nonconsecutive patients scheduled to undergo angioplasty from April 2009 to June 2011 were selected for the study. Of the 25 patients, 6 had stable angina, 8 had non–ST-segment elevation coronary syndrome, and 11 had evidence of myocardial ischemia. The exclusion criteria were recent (<72 hours) acute myocardial infarction, hemodynamic instability, renal insufficiency (serum creatinine >2.0 mg/dl), allergy to the contrast media, left main disease, ostial coronary artery lesion, bypass lesion, chronic total occlusion, and a tortuous vessel. Each of the selected patients underwent coronary angiography followed by the acquisition of 2 pullback images using FD-OCT with a minimum length of 18 mm (pullback 1, and, 5 minutes later, pullback 2). The optical coherence tomographic images were obtained in a coronary artery that was not found to be significantly diseased at angiography (diameter stenosis <50% on visual estimation). All patients provided written informed consent.
FD-OCT is a high-resolution intracoronary imaging technique with a maximum spatial resolution of 10 to 15 μm. The current generation C7 system (LightLab Imaging, Westford, Massachusetts) was used in the present study. The imaging catheters for FD-OCT were delivered over a 0.014-in. guidewire through ≥6F guiding catheters. For an effective clearing of blood from the imaging field, angiographic contrast medium was injected through the guiding catheter, as previously described, with image acquisition performed according to established methods.
In all patients, we performed a standard femoral catheterization approach. Unfractionated heparin was administered intravenously to maintain an activated clotting time >300 seconds. After coronary angiography, we positioned a 6F guiding catheter into the coronary ostium and advanced a standard 0.014-in. guidewire into the coronary artery. The imaging catheter for FD-OCT was advanced into the coronary artery to the segment of interest after administration of 200 μg intracoronary nitroglycerine. The blood was cleared by injection of iso-osmolar contrast (iodixanol 320, Visipaque, GE Healthcare, Dublin, Ireland) at 37°C with an injection pump (Acist, Bracco, Milan, Italy) through the guiding catheter. Two continuous motorized pullbacks (pullbacks 1 and 2) using FD-OCT were started as soon as the artery was cleared of blood. The images from each pullback were acquired at a speed of 20 mm/s from the same coronary segment until reaching the guiding catheter. The pullbacks were taken at an interval of 5 minutes without additional intervention between them. The coronary images acquired were saved on the OFDI system console and exported to a digital system for off-line analysis at an independent imaging core laboratory (Rome Heart Research, Rome, Italy).
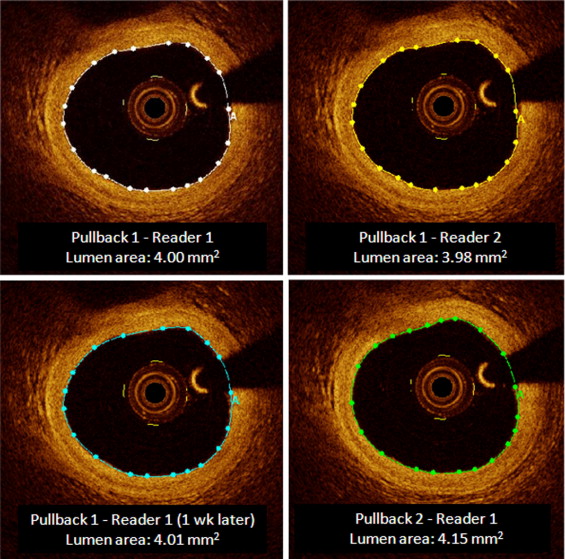
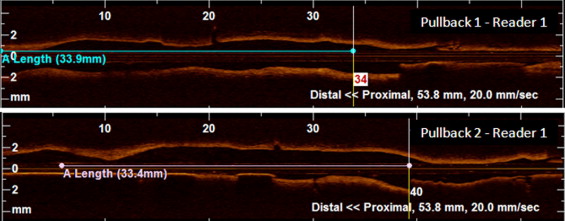
The analysis of the coronary images from FD-OCT was performed by 2 analysts (reader A and B) experienced in FD-OCT independently using a dedicated contour detection program (LightLab Imaging). First, we identified the coronary segment of interest in each pullback and verified the correspondence of the 2 pullbacks through side-by-side comparisons and using as reference landmarks the cross-sectional views of the side branches. After identifying the coronary segment in each pullback, we calibrated the measurements using the 6F (2-mm) catheter. In each cross-sectional coronary image, we calculated the lumen area using automatic contour tracing of the intima and the same detection program, with very occasional manual correction ( Figure 1 ). The length of the coronary segment was calculated from the number of cross-sectional frames taken of that segment ( Figure 2 ). To evaluate interobserver reproducibility, 2 independent readers (A and B) independently analyzed pullback 1. To determine intraobserver reproducibility, 1 reader (reader A) analyzed pullback 1 twice, with the second reading 1 week after the first. Finally, to assess interpullback reproducibility, 1 reader (reader A) analyzed pullbacks 1 and 2 during same work session. The analyses were conducted at the segmental (per-segment) level (thus including all frames obtained from the study subject) and frame (per-frame) level.
Correlation and bivariate regression analysis were performed to determine the association between different readings using both Pearson’s correlation and Spearman’s rho tests. In addition, Bland-Altman methods were used to obtain the bias estimates (reported as the mean and 95% bootstrapped confidence interval stemming from 1,000 samples each) and accompanying plots. Assuming an 8- ± 4-mm 2 lumen area and 20- ± 7-mm lesion length, 25 patients were deemed sufficient to achieve adequately small standard errors of the mean (0.8 mm 2 and 1.3 mm, respectively) and suitably precise 95% confidence intervals (6.4 to 9.6 mm 2 and 17.2 to 22.8 mm, respectively). Statistical significance was set at the 2-tailed 0.05 level, and p values unadjusted for multiplicity are reported throughout. Analyses were performed with SPSS, version 19 (IBM, Armonk, New York).
Results
We were able to acquire 2 separate coronary pullbacks using FD-OCT from each of the 25 patients in the study. The image quality of the pullbacks was excellent, with artifacts in <1% of the evaluated images. The manual correction of the automatic lumen area contour was performed in 25% of measurements from ≥1 reader. No imaging-related complications, such as coronary dissection, perforation, spasm, embolization, arrhythmia, or clinical adverse events, occurred. A total of 9,396 frames were included in the analysis, from which a longitudinal image of each patient coronary target lesion was reconstructed. The reproducibility of the coronary measurement analysis using FD-OCT in the present study was very high in all comparisons ( Table 1 ).
| Variable | Bland-Altman Bias ⁎ | Regression Analysis † (R Value, p Value) |
|---|---|---|
| Lumen area (mm 2 ) | ||
| Per-segment analysis | ||
| Interobserver | 0.001 (−0.012, 0.009) | 1.0, <0.001 |
| Intraobserver | 0.003 (−0.002, 0.009) | 1.0, <0.001 |
| Interpullback | 0.150 (−0.371, 0.086) | 0.982, <0.001 |
| Per-frame analysis | ||
| Interobserver | 0.001 (−0.001, 0.002) | 1.0, <0.001 |
| Intraobserver | 0.002 (0.001, 0.003) | 1.0, <0.001 |
| Interpullback | −0.091 (−0.139, −0.040) | 0.959, <0.001 |
| Length (mm) | ||
| Per-segment analysis | ||
| Interpullback | −0.200 (−3.00, 2.00) | 0.990, <0.001 |
⁎ Reported as mean (95% bootstrapped confidence interval stemming from 1,000 samples).
† Similar results for statistical significance and magnitude were obtained with Spearman’s correlation test.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


