To date, sparse data are available with regard to gender differences in plaque morphology and composition. The aim of the present report was to assess the differences in coronary plaque burden and composition in a noninvasive manner between women and men using multidetector computed tomographic angiography. The study population consisted of 416 patients (61 ± 13 years), with 148 women (36%). A stenosis of ≥70% in at least one coronary segment was found in 11% of women compared to 25% of men (p <0.0001). Overall, women presented with a significantly lower mean number of segments containing calcified plaques (1.43 ± 2.04 vs 2.25 ± 2.30, p = 0.004) and mixed plaques (1.67 ± 1.23 vs 2.25 ± 2.30, p = 0.05). No such relation was seen with noncalcified plaques (0.72 ± 1.01 vs 0.86 ± 1.06, p = 0.21). In addition, the assessment of the overall proportion of the composition of plaque burden revealed relatively more noncalcified (40% vs 28%), less calcified (38% vs 43%), and mixed (23% vs 28%) plaques in women than in men (p <0.0001). On multivariate analysis of the total plaque burden, the women had a 19% (95% confidence interval 11% to 28%, p <0.0001) greater relative distribution of plaque that was noncalcified compared to the men, and the overall plaque burden was less likely to be calcified (p = 0.006) or mixed (p = 0.019). Similar results were seen in younger and older subjects. In conclusion, gender differences exist, not only in the atherosclerotic disease burden, but also in the underlying plaque composition. Women tended to have more exclusively noncalcified plaque and were less likely to have calcified or mixed plaques compared to men. Future studies are needed to elucidate whether these underlying differences in plaque composition might explain the reduced risk of cardiac events in women.
The advent of multidetector computed tomographic angiography (MDCTA) has provided the ability to obtain comprehensive information regarding the location, severity, and characteristics of coronary atherosclerotic plaques, such as noncalcified, calcified, and mixed plaques. Coronary atherosclerotic plaque composition, rather than the plaque size or the degree of coronary artery stenosis, has been shown to be an important determinant of the evolution and disruption of the plaque. The greater coronary artery disease (CAD) event rates in men compared to women could be a result of the differences in coronary plaque burden and composition. Therefore, understanding the gender differences in plaque characteristics might be vital in understanding the gender-related differences in CAD. Thus, the purpose of the present study was to evaluate whether gender differences in the extent and composition of coronary plaques could be observed using coronary MDCTA.
Methods
We evaluated 416 consecutive, symptomatic patients with an intermediate to high risk of CAD who had been referred for MDCTA. The institutional review board committee board of the Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center (Torrance, California) approved the study protocol and consent form. MDCTA was requested for indications that included chest pain, shortness of breath, abnormal or equivocal stress test findings, cardiomyopathy, congestive heart failure, and syncope. Most patients presented for an evaluation of chest pain (346 of 416 [83%]). No gender differences were seen in the indication for MDCTA. In addition, none of the patients had had previous myocardial infarction or known CAD. The baseline demographic data, a history of hypertension, hyperlipidemia, and diabetes mellitus, smoking, and a family history of CAD were collected for all patients.
All multidetector computed tomographic angiographic scans were performed with a 64-detector row Lightspeed VCT scanner (GE Healthcare, Milwaukee, Wisconsin). All patients were in normal sinus rhythm at MDCTA. The patients presenting with a baseline heart rate >65 beats/min were administered oral β-blocker therapy as the preferred method for slowing the heart rate. When necessary, intravenous metoprolol was administered to a total possible dose of 40 mg to achieve a heart rate at rest of <65 beats/min. All patients eligible for MDCTA underwent scanning, irrespective of whether the heart rate goal of <65 beats/min had been achieved. After a scout X-ray of the chest (anteroposterior and lateral), a timing bolus (using 10 to 20 ml of contrast) was performed to detect the interval to optimal contrast opacification in the axial image at a level immediately superior to the ostium of the left main artery. Nitroglycerin 0.4 mg sublingually was administered immediately before contrast injection. During MDCTA, 80 ml iodinated contrast was injected using a triple phase contrast protocol (60 ml iodixanol, followed by 40 ml of a 50:50 mixture of iodixanol and saline, followed by a 50-ml saline flush). Retrospective electrocardiographic gated helical contrast-enhanced MDCTA was performed, with scan initiation 20 mm above the level of the left main artery to 20 mm below the inferior myocardial apex. The scan parameters were 64 × 0.625 mm collimation, tube voltage 120 kV, effective mA 350 to 780 mA. Radiation-reduction algorithms using electrocardiographic modulation were used to reduce the radiation exposure (mA) during systole and end-diastole. After scan completion, multiphasic reconstruction of the multidetector computed tomographic angiographic scans was performed, with reconstructed images from 70% to 80% by 5% and 5% to 95% by 10% increments. The multidetector computed tomographic angiographic images were reviewed by 2 experienced observers who were unaware of the patients’ clinical history. A high degree of agreement was observed (98%); in the case of disagreement, a final verdict was reached by consensus with a third experienced reader. All images were evaluated on a 3-dimensional image analysis workstation (GE Advantage Workstation, GE Healthcare). The coronary arteries were scored using a 15-segment American Heart Association coronary artery classification, as previously described. An overall assessment of image quality and coronary supply dominance was performed on the subject level. For each coronary segment, the readers assessed whether the coronary segments were evaluable. The segments were evaluated for the presence or absence of coronary plaques using axial images and curved multiplanar reconstruction. One coronary plaque type was assigned per segment. The plaques were defined as structures >1 mm 2 within and/or adjacent to the vessel lumen that could be clearly distinguished from the lumen and surrounding pericardial tissue. Plaques occupied by calcified tissue for >50% of the plaque area (density >130 Hounsfield units on native scans) were classified as calcified, plaques with <50% calcium were mixed, and plaques without any calcium were classified as noncalcified lesions. The calcified area was assessed manually.
To assess the independent relation of the different plaque subtypes with the degree of coronary stenosis, we performed linear regression analysis (with the total number of segments involved with plaque subtypes as the dependent variable) and logistic regression analysis (≥3 segments involved with plaque subtypes as the dependent variable). As a first step, we performed univariate analysis, followed by multivariate analysis, taking into account age, hypertension, diabetes mellitus, smoking, family history of coronary heart disease, hypercholesterolemia, body mass index, and lipid-lowering medications. A p value of <0.05 was considered statistically significant. All statistical analyses were performed using Stata, version 8.0 (StataCorp, Austin, Texas). The investigators had full access to the data and take full responsibility for its integrity. All investigators have read and agreed to the report as written.
The study population consisted of 416 symptomatic (mean age 61 ± 13 years, 36% women) patients who had undergone coronary MDCTA for assessment of underlying CAD. Table 1 lists the study population characteristics according to gender. Women were more likely than men to report diabetes mellitus and a family history of CAD (p <0.05). However, no statistically significant differences between the men and women were observed in age, prevalence of hypertension, hypercholesteremia, cigarette smoking, or obesity ( Table 1 ).
| Characteristic | Women (n = 148) | Men (n = 268) | p Value |
|---|---|---|---|
| Age (years) | 62 ± 13 | 60 ± 13 | 0.18 |
| Diabetes mellitus | 19% | 12% | 0.04 |
| Hypertension ⁎ | 47% | 39% | 0.11 |
| Hypercholesterolemia † | 55% | 55% | 0.97 |
| Smoker | 5% | 6% | 0.70 |
| Family history of premature coronary artery disease | 56% | 45% | 0.03 |
| Body mass index (kg/m 2 ) | 28 ± 6 | 28 ± 5 | 0.90 |
| Lipid-lowering medication | 17% | 16% | 0.82 |
⁎ Defined as systolic blood pressure ≥140 mm Hg and/or diastolic blood pressure ≥90 mm Hg and/or blood pressure-lowering medication.
† Defined as elevated total cholesterol, low-density lipoprotein, or triglycerides and/or low high-density lipoprotein.
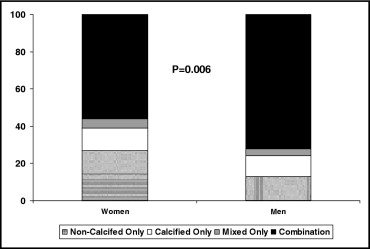
In our study participants, CAD was completely absent on coronary MDCTA in 51 (12%); a feature more likely in women than in men (23% vs 6%, p <0.0001). In the remaining 365 patients (88%) with underlying CAD, 63 (17%) had exclusively noncalcified plaques, 42 (11%) had exclusively calcified plaque, and 16 (4%) had mixed plaque. Most patients had a combination of the 3 plaque subtypes (n = 244, 67%). As shown in Figure 1 , women were more likely to have exclusively noncalcified plaque (27% vs 13%) and less likely to have a combination of plaque subtypes (56% vs 72%). As listed in Table 2 , women were less likely to have at least one coronary segment with a luminal diameter stenosis of ≥70% (12% vs 25%, p <0.0001) and were less likely to have significant stenosis involving 2 to 3 vessels.
| Characteristic | Women (n = 148) | Men (n = 268) | p Value |
|---|---|---|---|
| Narrowing >70% in diameter | 17 (12%) | 66 (25%) | <0.0001 |
| Maximal diameter stenosis | <0.0001 | ||
| No plaque | 34 (23%) | 17 (6%) | |
| 1–49% | 81 (54%) | 156 (58%) | |
| 50–70% | 16 (11%) | 29 (11%) | |
| >70% | 17 (12%) | 66 (25%) | |
| Narrowed coronary arteries | <0.0001 | ||
| 0 | 131 (88%) | 202 (75%) | |
| 1 | 10 (6%) | 45 (17%) | |
| 2 | 6 (4%) | 15 (6%) | |
| 3 | 1 (1%) | 6 (2%) |
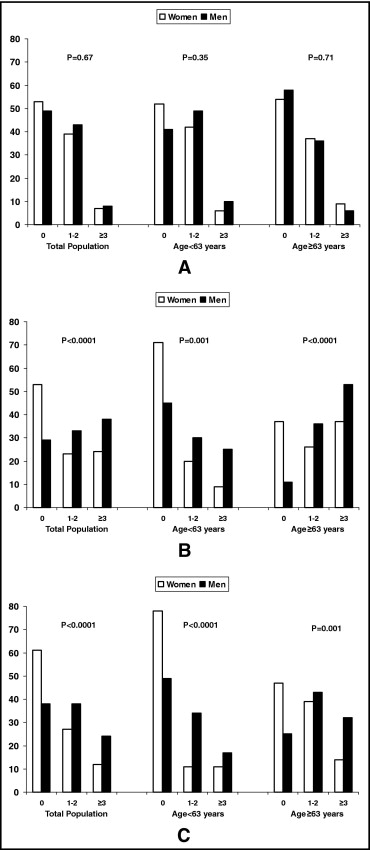
Overall, women presented with a significantly lower mean number of segments containing calcified plaques (p = 0.004) and mixed plaques (p = 0.05). However, no such relation was seen with noncalcified plaques (p = 0.21). As shown in Figure 2 , no difference in the distribution of coronary segments (0, 1 to 2, ≥3) with noncalcified was observed between the genders, with similar results when stratified according to median age (<63 and ≥63 years). Examination of the distribution of calcified and mixed plaques ( Figure 2 ) revealed that the proportion of women with ≥3 segments was much lower than that of men (p <0.0001). Although we observed no differences in the total number of coronary segments with noncalcified plaque according to gender, the relative distribution of plaque types was significantly more likely to be noncalcified and less likely to be calcified and mixed in women. These differences persisted when stratified according to the median age of the study population ( Figure 3 ).