Described herein are 10 patients who underwent cardiac transplantation (CT) for severe chronic systolic heart failure resulting from cardiac sarcoidosis. None had the diagnosis of sarcoidosis established before CT except for the 3 patients who earlier had had a portion of left ventricular wall excised for insertion of a left ventricular assist device and non-caseating granulomas were present in the removed myocardium. Although none of the 10 patients had significant narrowing of any of the epicardial coronary arteries, all had focal scarring of the walls of the left and right ventricles and ventricular septum and all had dilated ventricular cavities. The patients with the most ventricular wall scarring tended to have the fewest sarcoid granulomas in the ventricular walls. Two patients had no sarcoid granulomas in the excised heart although one did have typical sarcoid granulomas in the portion of left ventricular wall excised to insert a left ventricular assist device. Patients with cardiac sarcoidosis severe enough to warrant CT had characteristic cardiac ventricular morphologic findings, and no dysfunction of other non-cardiac organs, making clinical diagnosis of cardiac sarcoidosis rather difficult.
Although sarcoidosis of the heart has been recognized for over 70 years, most reports have appeared in the last 30 years. The condition continues to fascinate physicians because of its multiple modes of presentation—ventricular arrhythmias with or without cardiac arrest, various forms of heart block, heart failure, mitral regurgitation, left ventricular aneurysm—and its difficulty in diagnosis. Single case reports on the topic continue to appear as well as frequent reviews. In the last 2 decades a number of patients with cardiac sarcoidosis have undergone cardiac transplantation (CT) and few of them have had the condition diagnosed before CT or at least before cardiac biopsy (including the histologic examination of a portion of the left ventricular wall excised for insertion of a left ventricular assist device) ( Table 1 ). Since 1993, we have studied the hearts of 10 patients who underwent CT for severe chronic heart failure found to be the result of cardiac sarcoidosis. Our purpose was to subjectively quantify the relative density of the cardiac non-caseating granulomas in the myocardium and the extent and characteristics of the resulting scarring in the walls of the cardiac ventricles.
| First Author (Reference) | Year of Publication | Total CT (Years of CT) | No. (%) With Sarcoidosis | Ages of S Patients (Years) | F/M | W/B | Dx S Before CT | Extra Cardiac Sarcoid | Died | Cardiac Sarcoid Recurrence |
|---|---|---|---|---|---|---|---|---|---|---|
| Zaidi | 2007 | 38,230 (1987–2005) | 65 (0.2%) | 4–71 (m 45) | 25/40 | 44/19 | — | — | 16 | — |
| Miliman | 2008 | 250 (1990–2006) | 4 (2%) | 25–57 | 3/1 | 4/0 | 1 | 0 | 2 | 0 |
| Luk | 2009 | 296 (1987–2006) | 6 (2%) | — | — | — | 1 | — | — | — |
| Chang | 2012 | 411 (2003–2011) | 5 (1%) | 31–40 | 1/4 | — | 1 | 0 | 0 | 0 |
| Akashi | 2012 | 825 (1997–2010) | 14 (2%) | 42–67 | 7/7 | 5/7 | 6 | 7 ∗ | 6 | 2 |
| Totals | 40,012 | 94 (2.3%) | 4–67 | 36/52 | 53/26 | 9/1,782 | 7 | 24/88 (27%) | 2/23 (9%) |
Methods
The explanted hearts were sent to the surgical pathology division of the Baylor University Medical Center department of pathology. All hearts were examined and described by WCR and, after “cleaning” and fixation in formalin, weighed, and opened by him. At least 5 sections from the walls of the cardiac ventricles (endocardium through to epicardium) were processed, stained, and examined. From each paraffin block, 2 sections were cut: one was stained by both hematoxylin/eosin and the other by Masson, and each was examined by WCR. The medical records were then examined by MSC, JMK, and WCR.
The quantity of scarring in the left ventricular free wall, ventricular septum, and right ventricular free wall was graded subjectively by WCR on a scale of zero to 4+. Likewise, the density of sarcoid granulomas in the ventricular myocardium was graded zero (none seen) to 4+ (granulomas present in virtually all microscopic fields magnified ×40).
Results
From January 1993 through June 2013, a total of 346 isolated CTs were performed at Baylor University Medical Center. Of them, examination of the explanted hearts disclosed that 10 (3%) had cardiac sarcoidosis. Pertinent clinical and cardiac morphologic findings in them are summarized in Table 2 . Their ages at the time of CT ranged from 38 to 55 years (mean 48); 6 were women and 4 were men; 4 of 6 women were black and all 4 men were white. Symptoms of cardiac dysfunction in the 10 patients were present from 1 to 15 years (mean 7). Of the 10 patients, electrocardiograms before CT were available to examine in 9; of the 5 without a pacemaker, total 12-lead QRS voltage varied from 74 to 168 mm (1 mm = 1 millivolt) (mean 132) ( Table 2 ). Body mass index (10 patients) ranged from 19.0 to 32.0 kg/m 2 (mean 25.3). The lowest left ventricular ejection fractions ranged from 10% to 20% (mean 16). Three patients at the time of CT had a left ventricular assist device (Nos 6, 7, and 8, Table 2 ).
| Patient | Age at CT (Years) | Race | Age at Onset of Symptoms (Years) | Duration of Symptoms (Years) | Total 12-lead QRS Voltage (ECG) | ECG Date | BMI (kg/m 2 ) | Pressures (mm Hg) | CI (L/min/m 2 ) | Lowest LVEF (%) | LVAD | Date of CT | HW (g) | Largest Diameter (cm) | Grossly Visible Scar (0–4+) | Density Of LV Sarcoid Granulomas (0–4+) | Figure Number | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PA (s/d) | RV (s/d) | RA (Mean) | LV (s/d) | Aorta (s/d) | LV | RV | LV | VS | RV | |||||||||||||||
| WOMEN | ||||||||||||||||||||||||
| 1 | 50 | B | 38 | 12 | 113 ∗ | 10/05/2008 | 27.0 | — | 43/— † | 10 † | — | — | — | 20 | 0 | 1/28/2012 | 440 | 7.5 | 4.0 | 3+ | 2+ | 1+ | 4+ | 1 |
| 2 | 52 | B | 48 | 4 | — | — | 28.7 | 59/28 | 59/15 | 9 | 115/34 | 115/79 | 1.7 | 20 | 0 | 9/4/2010 | 440 | 5.5 | 2.0 | 3+ | 2+ | 1+ | 1+ | 2 |
| 3 | 56 | W | 55 | 1 | — | — | 25.7 | — | — | — | 109/33 | 104/79 | — | 15 | 0 | 10/30/2009 | 445 | 5.5 | 3.5 | 4+ | 4+ | 4+ | 4+ | |
| 4 | 58 | W | 54 | 4 | 74 | 3/10/2012 | 26.4 | 20/11 | — | 8 | — | — | 2.2 | 20 | 0 | 3/10/2012 | 560 | 5.0 | 2.5 | 4+ | 4+ | 2+ | 3+ | 3,6 |
| 5 | 62 | B | 49 | 13 | 168 | 2/18/2013 | 19.0 | 36/14 | 62/— † | 20 † | — | — | 2.6 | 10 | 0 | 3/16/2013 | 600 | 7.5 | 6.0 | 4+ | 0 | 2+ | 0 | 4 |
| 6 | 59 ‡ | B | 55 | 4 | — | — | 20.8 | 44/21 | — | — | — | — | 1.8 | 20 | + | 7/9/2006 | 370 | 5.0 | 7.5 | 2+ | 2+ | 0 | 4+ | 6 |
| MEN | ||||||||||||||||||||||||
| 7 | 50 ‡ , § | W | 47 | 3 | 147 | 1/02/2005 | 24.7 | 97/45 | 92/15 | 11 | — | — | 1.7 | 10 | + | 1/14/2005 | 605 | 7.0 | 2.5 | 4+ | 1+ | 0 | 0 ‖ | |
| 8 | 52 ‡ , § | W | 48 | 4 | 158 ∗ | 11/22/2002 | 21.6 | 51/23 | 49/6 | 6 | — | — | 1.6 | 20 | + | 7/8/2005 | 440 | 5.0 | 3.5 | 2+ | 2+ | 0 | 4+ | |
| 9 | 54 ¶ | W | 41 | 13 | — | — | 27.5 | 32/14 | 32/12 | 8 | — | — | 2.1 | 10 | 0 | 9/5/1999 | 510 | 9.0 | 9.0 | 1+ | 1+ | 1+ | 4+ | |
| 10 | 63 | W | 48 | 15 | — | — | 32 | 23/8 | 24/7 | −1 | — | — | 1.6 | 15 | 0 | 1/6/2013 | 470 | 6.0 | 4.0 | 3+ | 1+ | 4+ | 1+ | 5 |
∗ Electrocardiogram recorded 3 or 4 years before CT.
‡ These 3 patients were included in a previous report ( Am J Cardiol 2009;103:110–114) .
§ Diagnosis of cardiac sarcoid made from histologic study of “left ventricular core” excised for insertion of a left ventricular device.
‖ Sarcoid granulomas present in the left ventricular “core” but not in the excised native heart.
¶ Case previously published ( Am J Cardiol 2002;89:1447–1450) .
The weights in the hearts in the 4 men ranged from 440 to 605 g (mean 506) and in the 6 women, from 370 to 600 g (mean 476). The maximal internal dimension of the left ventricular cavity ranged from 5.0 to 9.0 cm (mean 6.3); the maximal internal diameter of the right ventricular cavity (right ventricular free wall to ventricular septum at posterior wall at the base) ranged from 2.0 to 9.0 cm (mean 4.5).
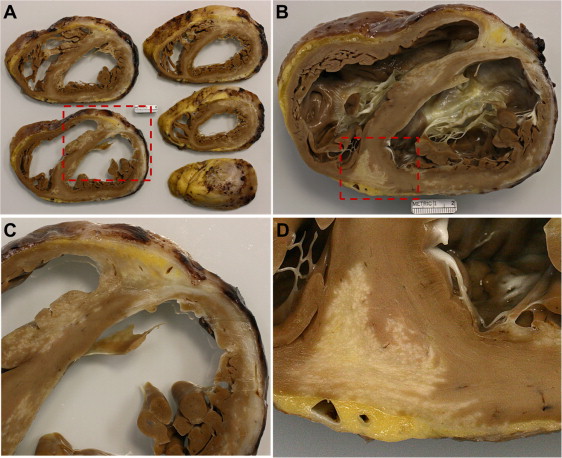
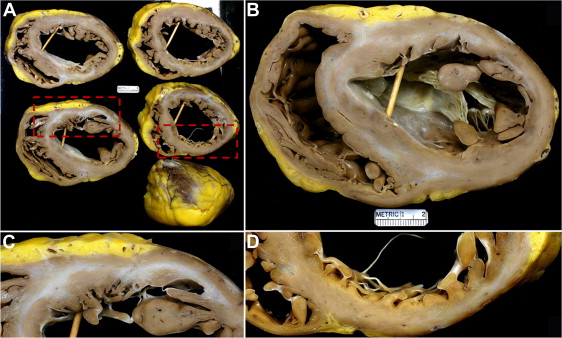
Grossly visible scars were present in the left and right ventricular free walls and in the ventricular septum in all 10 patients (Figures 1 to 4 ) and none of the 10 patients had narrowing of any significant degrees in any of the epicardial coronary arteries. The left ventricular scars were most often transmural but often were also or only subepicardial (outer one-half of the myocardial wall). Scars in the right ventricular free wall were transmural (full thickness scarring). Scars in the ventricular septum also varied in extent: some were transmural and when not were often centrally located in the septum or in the right ventricular half rather than the left ventricular half of the septum. No grossly visible scars or other lesions were observed in the walls of either the right atrium or left atrium, but much of these walls were retained in the recipient to connect to the donor heart. No patient had sarcoid lesions in the cardiac valves, coronary arteries or subepicardial adipose tissue.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


