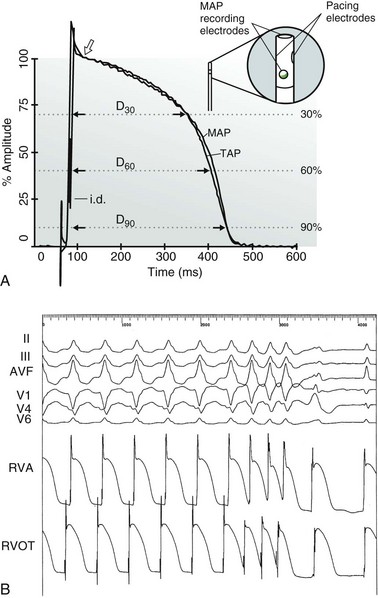
68 Recording of monophasic action potentials (MAPs) by contact electrode catheter can be performed easily and safely in the human heart. Unlike body surface electrocardiographic (ECG) recordings or standard endocardial electrograms, which produce a summative or derivative view of the heart’s electrical activity, MAP recordings provide local information about the actual cellular depolarization and repolarization process of myocardial tissue. By giving clinical investigators a more direct view of human myocardial electrophysiology in situ, in both normal and disease states, MAP recordings serve as an important bridge between cellular and bedside electrophysiology. This chapter discusses the methods and presents selected, clinically pertinent applications of MAP recordings. The genesis of MAPs by contact electrode technique has been described in a review1 and has been discussed in more recent work.2 The design of the contact electrode catheter tip is schematically illustrated in Figure 68-1, A (inset). The exploring hemispherical MAP electrode forms the catheter tip and is made of nonpolarizable silver–silver chloride (Ag-AgCl) or similar matrix. Another Ag-AgCl electrode is located 5 mm proximal to the tip (close bipolar design) and serves as the MAP reference electrode. When the catheter tip is directed perpendicularly or at some angle of it against the endocardium, depolarization is confined to a small area subjacent to the tip electrode. The distal portion of the catheter shaft incorporates a flat spring wire that ensures stable contact between the tip electrode and the endocardium throughout the cardiac contraction-relaxation cycle, and also provides superior torque control. The tip electrode lead is connected to the positive input, and the proximal electrode lead is connected to the negative input, of the recording system. Figure 68-1 A, Simultaneous recordings of intracellular transmembrane action potential (TAP) and extracellular monophasic action potential (MAP) show high congruence. Repolarization is labeled at 30%, 60%, and 90% of the return from plateau to resting potential. Inset: Contact electrode catheter design for recording MAPs from endocardium in patients or large animals. Shown is the MAP-pacing combination catheter, which includes small pacing electrodes located 2 mm proximal to the catheter tip in an orthogonal position. This catheter incorporates a bidirectional steering feature (not shown). B, MAP recordings from two right ventricular (RV) sites along with body surface electrocardiogram during programmed electrical stimulation. Pacing is performed at the RV outflow tract (RVOT). Note small pacing artifacts immediately preceding the MAP upstrokes. Extra-stimulus responses show increasing separation between stimulus and MAP upstroke. RVA, RV apex. (A, From Franz MR, Burkhoff D, Yue D, Lakatta E: In vitro validation of a new cardiac catheter technique for recording monophasic action potentials. Eur Heart J 7:34-41, 1986; inset, adapted from Franz MR, Chin MC, Sharkey HR, et al: A new single catheter technique for simultaneous measurement of action potential duration and refractory period in vivo. J Am Coll Cardiol 16:878-886, 1990.) Unlike in conventional electrode catheters, the pacing electrodes are not distal but are mounted in orthogonal position halfway between the distal (tip) and proximal (reference) MAP electrode. This electrode configuration provides for extremely low stimulus capture thresholds (0.02 to 0.25 mA; mean, 0.09 mA), resulting in minimal interference between the pacing artifact and the MAP signal. This feature facilitates precise and simultaneous determinations of both the action potential duration (APD) and the effective refractory period (ERP) at the same myocardial site (Figure 68-1, B). The “Franz” contact electrode MAP catheter records the relative voltage time course of cardiac cell membranes with high fidelity (see Figure 68-1, A, inset). It does not, however, reproduce the full magnitude of the transmembrane action potential (TAP), nor does the MAP render information on the absolute rise velocity (Vmax) of the TAP upstroke. The beginning of the MAP is defined as the instance of fastest rise time of the MAP upstroke. Because the asymptotic end of repolarization makes precise measurement of total MAP duration difficult, the MAP duration usually is determined at a repolarization level of 90% (or another fraction) with respect to the MAP amplitude. The MAP amplitude is best defined as the distance from the baseline to the crest of the MAP plateau, not its upstroke peak. As an alternative, use of the intersection between the diastolic baseline and a tangent placed on phase 3 repolarization has been suggested; this approach may produce more arbitrary results, depending on the slope of final repolarization. The contact electrode MAP catheter with pacing capability can be used for routine electrophysiological studies, including programmed electrical stimulation. The MAP-pacing combination catheter offers several advantages over conventional quadripolar catheters: (1) The local endocardial activation time is indicated by the MAP upstroke, which is sharp and unambiguous, in contrast with the often multiphasic deflections obtained with conventional catheters, thereby making measurements of local activation time easier and more accurate (see Figure 68-1, B). (2) Pacing thresholds with the MAP-combination catheter are extremely low and stimulus artifacts are minimized dramatically, providing unobscured local myocardial responses (see Figure 68-1, B). This feature also is useful for differentiating local stimulus response latency from “downstream” conduction delays. (3) Because local repolarization is visualized by the MAP, the ERP, which usually coincides with 75% to 85% repolarization, can be anticipated and confirmed quickly without prolonged extra-stimulus scanning. This facilitates visualization of changes in the ERP that occur independently from changes in APD (see later). (4) MAPs are recorded only when the catheter tip electrode is in close contact with the endocardium. A stable MAP verifies stable tip-electrode contact, facilitates a constant stimulus threshold, and avoids confusion with intracavitary potentials, as might be the case with conventional electrograms, when small signal amplitudes are the only way to suspect insufficient tissue contact. (5) With conventional electrophysiological catheters, fractionated, double, or late potentials have been observed and interpreted as markers of abnormal conduction in scarred myocardium, which is believed to be a substrate for reentry tachycardia; however, concerns that some fractionated electrograms represent artifacts have been raised. Comparisons between MAP signals and conventional electrograms can be helpful in identifying the nature of these fractionated electrograms (see later). A list of clinical applications of MAP recordings is given in Box 68-1. Box 68-1 Clinical Applications of Monophasic Action Potential (MAP) Recordings • Effects of antiarrhythmic drugs on APD and ERP/APD ratio • Repolarization abnormalities in congenital or acquired long QT syndromes and Brugada syndrome • Measuring dispersion of repolarization by MAP mapping techniques • Evaluation of T wave changes and memory • Myocardial ischemia detection and distinction between viable and nonviable myocardium • Distinction between VT and VF during ICD testing • Effects of rate and rhythm on APD in humans, including restitution curves • Detection of dominant frequency in atrial fibrillation
Monophasic Action Potential Recording
Monophasic Action Potential Recording
Monophasic Action Potential Recording Devices
Monophasic Action Potential Recording Catheters for the Clinical Electrophysiology Laboratory
Accuracy of Monophasic Action Potential Recordings
Clinical Applications of Monophasic Action Potential Recording
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Monophasic Action Potential Recording
