Despite advances in imaging techniques and the molecular characterization of lung tumors described elsewhere in this volume, the histopathology of lung cancer remains the basis for diagnosis and treatment of the disease and is essential for the interpretation of imaging studies and molecular analyses. Histopathology has recently taken on added importance as it has been recognized that targeted agents affect specific lung tumor subtypes differently and that successful treatment may depend on histological distinctions that have been previously unrecognized or ignored. Historically, the classification of lung cancer rested on the expertise of individual pathologists but in 1967, an international panel was first assembled through the World Health Organization (WHO) to create a standard nomenclature for lung cancer. This classification with its periodic revisions has become the most widely used standard for diagnosis and treatment and is provided in Appendix A. The most recent edition of the WHO morphological classification was published in 2004 and is more comprehensive than previous editions’ description of the classification, taking into account molecular data as well as morphology.1 The purpose of this chapter is not so much to recapitulate the details of the WHO classification but rather to provide an understanding of the main categories of lung carcinoma, to highlight potential pitfalls in histopathological diagnosis of lung cancer, to summarize current information on molecular properties and cellular origin of individual lung tumor types, to relate pathology to biological behavior, and to provide review guidelines for reporting and pathological staging of lung cancer.
Nearly all lung cancers exhibit the morphological and molecular features of epithelial cells (described later) and are accordingly classified as carcinomas. The cells of origin of virtually all lung cancers reside in the epithelial lining of the airways. As more is learned about the origin of lung carcinoma, it is increasingly clear that the biology of lesions arising in the central airways is distinct from that of peripheral airway lesions. In addition, there are important distinctions between tumors from the two sites in histopathological appearances, molecular profiles, and diagnostic approaches. While the dichotomy between central and peripheral is not a sharp one, it is nevertheless useful to consider tumors of the central airways separately from peripheral tumors.
TUMORS PREDOMINANTLY OF THE CENTRAL BRONCHI
In this chapter, we use the term central airway lesions to refer to tumors and premalignant conditions predominantly arising proximal to the terminal bronchiolar and alveolar epithelium. Surprisingly, little information is available on the cells from which central airway carcinomas arise. It might be expected that since the high risk posed by tobacco exposure has been known for many years, the earliest changes in the airway lining cells would by now be well known and the subject of interventional trials. That this is not the case is because of the macroscopic invisibility of early carcinoma and its precursor lesions, to the inaccessibility of the lower airway epithelium to direct inspection and serial sampling and to the great extent of the lower airway epithelial surfaces. It has nevertheless been known for many years that, in the central airways, a distinct series of changes of variable severity may be seen in the airways of smokers. Typically these lesions, described in detail later in the chapter, have been regarded as precursors of squamous carcinoma but there is evidence that they may also represent precursors of other histological types of central airway carcinoma, including undifferentiated large and small cell lung carcinomas (SCLC).
Central Airway Precursor Lesions Lung carcinoma, like tumors in other organs, is thought to arise from a stepwise series of molecular and cellular alterations in precursor cells. The first studies to demonstrate significant histological changes in the lower airways of the human population were the autopsy analyses of Auerbach and colleagues2 performed over 50 years ago. These studies consisted of serial cross sectioning of tracheobronchial tissue removed at autopsy from 1522 adult smokers and control nonsmoking patients without invasive carcinoma. Nearly 42,000 bronchial cross sections were evaluated and epithelial lesions consisting of atypical cells were found in 93% of sections from current smokers but in only 1.2% of sections from individuals who were never-smokers. Cellular abnormalities in smokers’ lungs were often multifocal and were independent of age, sex, place of residence, and the presence of pneumonia. A significant number of individuals who were former smokers in this study also had cellular abnormalities, whereas they were rare in individuals who never smoked.3
Sputum Cytology and Risk Assessment Although these studies documented the prevalence of cellular lesions in the lower airways at a single time point in smokers who did not have carcinoma, prospective confirmation that these lesions represent precursor lesions for carcinoma has been problematic. A major difficulty is a lack of any creditable intervention strategy that can be offered to individuals who are found to have dysplasia. In other organs, preinvasive lesions can be excised and this has been a successful strategy in cervix and colon where screening has proven successful in reducing the incidence and mortality of invasive carcinoma.4,5
The most analogous studies in the lung are the lung cancer screening trials of the 1970s and 1980s. In these studies, the effectiveness of sputum cytology as a screening tool was evaluated in 21,000 subjects at Sloan-Kettering Medical Center and the Mayo Clinic. Spontaneous sputa were evaluated by conventional cytological criteria for the presence of carcinoma. Cytology proved to be an insensitive tool for detection of lung cancer. Only 41% of subjects were sputum positive among those who had carcinoma at an initial (prevalence) screen and 17% with carcinoma in subsequent (incidence) screenings. In the Mayo Clinic project, no effect on mortality could be demonstrated by chest radiograph or sputum cytology performed quarterly for 6 years. The only positive trend resulting from these interventions was a slightly improved median survival for screen-detected stage I carcinomas in comparison to those detected outside the screened group, a difference that was not statistically significant.6
The failure of sputum and radiograph screening to reduce mortality from lung cancer has largely been attributed to overdiagnosis bias.7,8 Overdiagnosis bias refers to the detection of tumors through screening that, even if undetected, would not have affected mortality. It implies either that death may occur from other causes before any mortality effect from screened tumors can occur, or that the detected tumors were indolent and would not have affected survival. The lack of impact of screening on overall mortality has lead to the proposal that small screen-detected tumors are biologically distinct from advanced tumors that are responsible for the high mortality in lung cancer. Small screen-detected tumor are postulated to have lower growth rates and different epidemiological associations than those of advanced lethal tumors and, moreover, may not be precursors of advanced lesions,9 as is widely believed. The morphological and biological features of screen-detected central airway tumors have been analyzed by Mayo pathologists.10 Only 86% of the screened tumors were unequivocally invasive with 14% regarded as preinvasive by one or more of the pathologists on the reviewing panel. Inclusion of preinvasive lesions in the outcome analysis may have contributed to overdiagnosis bias in the Mayo Lung Project and provides some biological basis for the outcome of the trial.
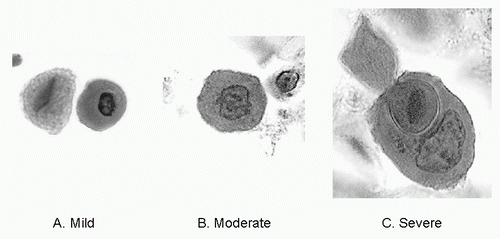
FIGURE 22.1 Dysplastic squamous cells in sputum. A: Mild dysplasia on the right consists of small rounded red cell with condensed nucleus and low N/C ratio. B: Moderately dysplastic orangophilic cell with large irregular nucleus and visible nucleolus. C: Carcinoma with large nucleus, high N/C ratio and visible nucleolus. Large cell appears to be ingesting smaller one. (See color plate.)
One crucial difference between the lung cancer screening trials and screening practices for colon and cervix is that the latter target preinvasive lesions rather than fully developed invasive carcinomas. A similar approach has not been fully explored in lung cancer. The significance of less than fully malignant cells in the sputum (Fig. 22.1) has recently been evaluated.11,12 These studies have shown that cytologic atypia is a marker for increased lung cancer risk. The association of sputum atypia with lung cancer increases with the severity of the atypia, with short interval between sputum collection and with squamous tumor histology. Higher-grade cytological changes thus seem to arise from late events in the central airways. Whether sputum atypia can be a useful indicator for the presence of premalignant dysplasia in the central airways, whether the presence, grade, and extent of dysplasia predicts invasive carcinoma, and whether meaningful interruption or delay in neoplastic progression is possible when premalignant changes are identified are questions currently being investigated using new methods for visualizing and directly sampling bronchial mucosa for histological assessment.
HISTOLOGY OF SQUAMOUS DYSPLASIA
Because premalignant lesions and early carcinomas are not easily recognized by white-light bronchoscopy, the stimulus for evaluating the lower airways to identify lower airway neoplasia by this method has not been great. Only recently has it been possible to detect premalignant lesions using fluorescence bronchoscopy as described in this volume and elsewhere.13,14
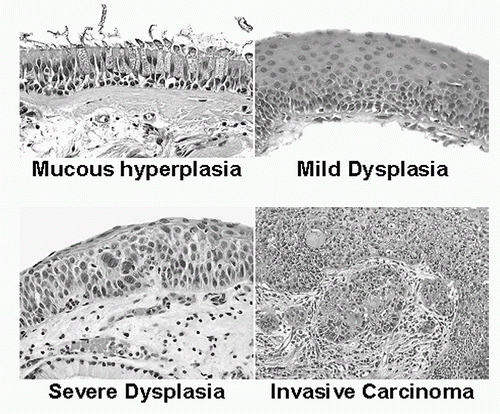
This technical advance has engendered a need for a reproducible and less descriptive classification of bronchial premalignancy than that used in the earlier studies of Auerbach. The WHO pathology panel has recognized this need and has provided a suggested classification based largely on the earlier work of Saccomanno and illustrated in Figure 22.2. The classification is based on cellular changes that occur in the epithelium, which consist of a transformation of bilayered mucociliary epithelium to squamous epithelium that is associated with varying degrees of alteration in nuclear irregularity and mitotic activity. The classification includes seven categories including histologically normal epithelium, basal cell hyperplasia and squamous metaplasia, mild, moderate, and severe dysplasia, and carcinoma in situ (CIS). Independent studies have indicated that this classification is reproducible15 and may be used in clinical trials targeting premalignant changes in the airways.
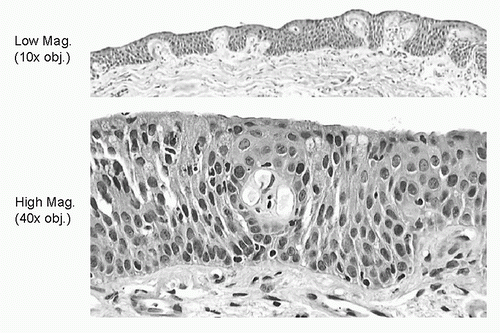
In addition to changes in the bronchial epithelium, changes in the stromal support tissues have also been described. Potentially, the most significant of these changes may be microscopic evidence neoangiogenesis that has been referred to as angiogenic squamous dysplasia (ASD).16 ASD is characterized by the sprouting of capillaries into dysplastic squamous mucosa (Fig. 22.3). These lesions are frequently multifocal, may persist for several years at the same bronchial sites and are preferentially associated with squamous carcinoma.17
Although areas of squamous dysplasia are now more readily identified in the central airways, the risk posed by dysplastic lesions discovered at bronchoscopy has not been quantified. What is known is that CIS is associated with progression to invasive carcinoma in many cases18 but not all and that CIS with aneuploidy in more likely to be associated in invasive carcinoma (discussed later).19 One form of squamous CIS exhibits a horizontal pattern of spread that may extend a considerable distance along the airway mucosa without invasion or metastasis.20 The prognosis in those few cases that have been reported has been excellent. The prognostic significance of lesser degrees of bronchoscopically detected dysplasia is not yet well defined but the association with invasive carcinoma is much weaker than with CIS.19 It is likely that lesser degrees of dysplasia persist for many years before undergoing sufficient genetic alteration to progress to invasive tumor.
FIGURE 22.2 Chronological sequences of cellular and molecular changes that may occur during central airway carcinogenesis. Although this sequence is rarely observed in a single individual, these changes are well described in the high-risk population and the sequence provides a useful way to conceptualize multistep carcinogenesis in the lung. At the cellular level, the earliest smoking-related changes may consist of mucous gland hyperplasia (shown), basal cell hyperplasia, or squamous metaplasia, which are not recognizably premalignant changes. The earliest cellular abnormalities that suggest premalignancy are squamous dysplastic changes that may range from mild-tosevere carcinoma in situ. The appearance of stromal invasion marks progression to fully established malignancy. (See color plate.)
FIGURE 22.3 Premalignant changes in the bronchial epithelium. Mucociliary cells are converted to squamous cells and may elicit and angiogenic stromal response shown at low maginfication (top) and high magnification (bottom). Nuclear irregularity with clearly visible nucleoli is present in the cells surrounding the vascular loop in the lower frame. (See color plate.)
Finally, nonsquamous atypias of the respiratory mucosa have recently been reported.21 In our experience, nonsquamous dysplasias of the central airways are less common and more difficult to recognize than squamous lesions. It will be important, however, to determine whether these lesions are significant predictors of nonsquamous carcinoma.
Immunohistochemical Changes in Bronchial Dysplasia Premalignant squamous lesions in the lower airways are associated with a constellation of changes in protein expression that can be demonstrated by immunohistochemical methods, including overexpression of cytokeratin 5/6 (CK5/6),22 epidermal growth factor receptor (EGFR),23,24 human epidermal growth factor receptor 2 (HER-2)/neu,24,25,26 and the cell cycle-associated protein Ki-67,24,27,28 fatty acid synthase,29 and MCM2.24,30 Loss of FHIT,31 p16,32 E-cadherin,33 and catenin33 has also been demonstrated. Nuclear p53 accumulation has been described in dysplasia32,34 but is usually focal and immunostained cells rarely have the robust signal present in tumors with homozygous mutation. Most of these immunohistochemical changes are first visible when normal mucociliary epithelium changes to squamous epithelium and do not visibly progress with the level of dysplasia. Exceptions to this rule are the biomarkers that are associated with cell proliferation. Generally, there is an increase in the level of expression of cell proliferation markers with increasing histological grade. Cyclin D1,32,35,36 cyclin E,37 PCNA,38 Ki-67,24,27,28 and MCM224,30 all increase with increasing grade of dysplasia, reflecting the increased proliferative capacity of more severely dysplastic cells. With the possible exception of proliferative immunohistochemical biomarkers, no single change in immunohistochemically demonstrable protein expression has to date added significantly to the information that can be gleaned from conventional histological examination.
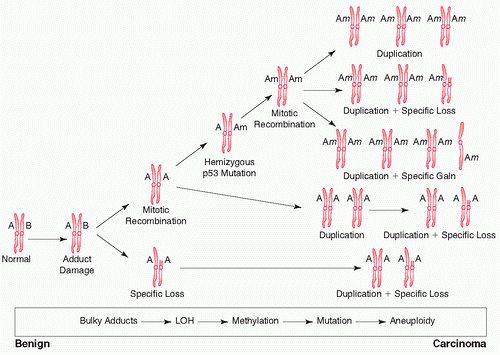
Genetics of Preneoplasia Underlying the morphological and immunohistochemical changes that occur in the airways is a multistep sequence of molecular and chromosomal events illustrated in Figures 22.4 and 22.5. The initial event in lung carcinogenesis is the formation of DNA adducts, the physical complexes between DNA, and the reactive metabolites in tobacco smoke and industrial pollutants.39,40,41 Among the most potent of the carcinogens are polycyclic aromatic hydrocarbons (PAH), aromatic amines, and metals. These compounds are largely metabolized to execrable products by cytochrome p450 and glutathione S transferase (GST). However, some small fraction of intermediates is highly reactive with DNA and forms bulky adducts with DNA in which the reactive metabolite is covalently bonded to specific DNA bases.40
FIGURE 22.4 Lung carcinogenesis is thought to proceed through the accumulation of genetic and chromosomal abnormalities depicted in this diagram in approximate chronologic sequence. One of the earliest events is bulky DNA adduct formation as a result of exposure to carcinogens in tobacco smoke and which is not visible at the chromosomal level. Adducts may interfere with DNA repair and mitosis resulting in mitotic recombination or partial chromosomal loss. Recombination could explain the nearly ubiquitous occurrence of LOH that occurs early in lung carcinogenesis. Gene methylation, mutation, further mitotic recombination, and a high level of chromosomal rearrangement (chromosomal instability) may then occur resulting the high level of aneuploidy that is present in many lung carcinomas. LOH, loss of heterozygosity. (Reproduced from Franklin WA, Hirsch FR. Molecular and cell biology of lung carcinoma. In: Sculier JP, Fry WA, eds. Malignant Tumors of the Lung. New York: Springer-Verlag, 2003:3-17.)
DNA adducts activate complex DNA repair mechanisms, which are not completely effective in removing adducts from damaged DNA. Unrepaired DNA bases may be bypassed by DNA polymerase, creating mutations that are transmitted to daughter cells. Mutations formed in this way tend to favor GC→TA transversions. Many of the genetic changes that ultimately appear in lung carcinomas are thus thought to originate from misrepaired DNA adducts.
Among these changes are allelic losses, easily demonstrated by a simple molecular test based on the measurement of the length of polymorphic tandem repeat sequences that exist throughout the genome. In these tests, chromosomal loci that normally harbor two different polymorphic alleles are assessed for loss of one (loss of heterozygosity [LOH]) or both of these alleles. Loss of both alleles (homozygous deletion) results in silencing of the gene while loss of a single allele (heterozygous loss) causes loss of gene expression if the retained allele is mutated or inactivated by methylation. Loss of genes that are important in controlling cell growth, apoptosis, or error DNA replication can impart a malignant phenotype to lung cells and much effort has been expended in trying to identify candidate tumor suppressor genes in dysplastic epithelium and invasive tumors.42
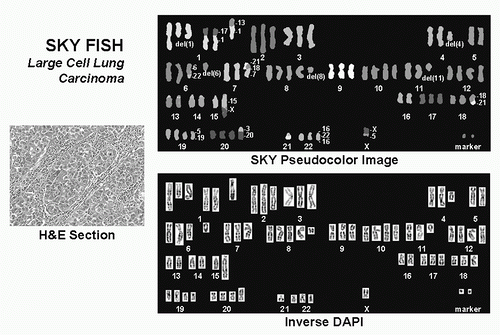
FIGURE 22.5 Chromosomal heterogeneity and instability. The high degree of chromosomal instability in lung carcinoma is reflected in numerous structural abnormalities that are visible through chromosomal imaging methods. Shown here is a spectral karyotype of a large cell undifferentiated carcinoma (H&E section). The SKY pseudocolor image of the karyotype provides a color code for each chromosome. In this figure, extra chromosomes 1, 2, 3, 4, 6, 7, 8, 9, 10, 11, 12, 18, 19, 20, and 22 are visible. A reciprocal translocation, several nonreciprocal translocations, deletions, and marker chromosomes are also present. FISH, fluorescence in situ hybridization; H&E, hematoxylin and eosin; SKY, spectral karyotyping. (See color plate.)
Allelic losses at loci throughout the genome have been demonstrated in premalignant bronchial mucosa and detailed consideration of specific allelic losses is reviewed elsewhere.43,44 Several conclusions may be drawn from LOH studies performed so far. First, many regions of allelic loss have been demonstrated in smoking damaged airways but few studies have demonstrated any effect of LOH on corresponding gene expression. Second, many loci demonstrate loss from the earliest exposure to tobacco smoke but allelic loss does not occur in individuals who have never smoked.45 Finally, no specific loss appears to be crucial for progress to malignancy but rather it is the accumulation of multiple losses that is most tied to malignant progression.46
The molecular mechanism responsible for allelic loss is not fully known. It has been suggested that bulky adducts resulting from DNA oxidation could affect repair of double-stranded DNA breaks and result in the recombination of homologous recombination of DNA strands during the repair process. Fluorescence in situ hybridization (FISH) studies have indicated an increase rather than a decrease in gene copy number occurs at sites of allelic loss,47 suggesting that tumor cells harbor multiple copies of the same allele and that gene dosage may in fact be increased. Allelic loss may result in functional loss of protein only when the retained allele is mutated or silenced by methylation.
A molecular property that distinguishes lung cancers and, to a lesser extent, premalignant lesions from normal bronchial cells is chromosomal instability, which is reflected as aneuploidy in tumor and premalignant cells. Aneuploidy is first detected in squamous dysplasia48 and in one recent study, aneuploidy was found in cultured bronchial epithelial of 26% of high-risk smokers.49 In invasive lung carcinomas, aneuploidy is nearly universal and involves multiple chromosomes.50 Aneuploidy has been found in lung cancer by classical cytogenetics methods51 but is more efficiently demonstrated by FISH. Numerical abnormalities have been demonstrated in every chromosome by FISH.52,53,54
New technologies such as spectral karyotyping (SKY) (Fig. 22.5) and comparative genomic hybridization indicate that not only are numerical chromosomal imbalances frequent but also structural chromosomal abnormalities such as translocations and amplifications are ubiquitous as well.55 This high degree of chromosomal instability may explain the extreme molecular and cellular heterogeneity of lung cancers as well as their adaptability and resilience in the face of chemotherapeutic treatment.
Patients with squamous as well as large and SCLC frequently harbor dysplastic squamous lesions in the central airways although the precise frequency in which this occurs is not known. There is also increasing evidence of genomic and phenotypic plasticity in invasive carcinomas, and tumors of mixed histological type are a frequent finding in the lung suggesting that tumor cells of many histological types could arise from a common progenitor. Molecular evidence indicates that lung tumors recapitulate ontological development,56,57 suggesting that central airway lesions of various histological types could represent arrested development at various stages in the same progenitor cells rather than origin from separate progenitor cell lineages.
Invasive Squamous Carcinoma of the Bronchus Squamous carcinomas are in the most common of the central airway tumors and are highly associated with smoking.58 Invasive squamous tumors are characterized by extension of malignant squamous cells beyond the basement membrane of the airway lining. Approximately 29% of lung cancers are of this histological type (Table 22.1).59 The diagnosis of squamous carcinoma and indeed of all non-small cell tumors has taken new importance with the recognition that new targeted agents may differentially affect non-small cell subtypes and it is therefore more important to recognize and report squamous lesions than in the past.
TABLE 22.1 Frequencies of Histological Types
Histological Type (Subtype)
% Total
Squamous carcinoma
29%
SCLC
20%
LCLC
9%
LNEC
2%
Adenocarcinoma
32%
-(Bronchioloalveolar)
3%
Others
12%
HISTOLOGY OF SQUAMOUS CARCINOMA
The histological features of squamous carcinoma are summarized and compared with other forms of lung cancer in Table 22.2. Invasion is recognized as angulated nests or individual tumor cells that have broken away from the surface epithelium and become embedded in the stromal tissues as shown in Figure 22.6. The invasive cells may form keratin pearls (KP) and intercellular bridges60 and may develop irregular areas of central necrosis described as geographic necrosis. Nuclear features include irregular nuclei and coarse chromatin. The cytoplasm may show clearing, most clearly seen in clear cell variant of squamous cell carcinoma, which can resemble vacuolization as might be seen in adenocarcinomas. Squamous tumors also elicit a variable stromal response consisting of loose fibroblastic tissue with an inflammatory component that may include plasma cells, macrophages, and lymphocytes. In more poorly differentiated carcinomas, there is less keratinization and intercellular bridges may be difficult to identify. Here, the overall epithelioid architecture of the tumor cells is important for diagnosis. In these cases, there may be maturation of cells from a basilar zone to a central area where there is loss of the typical verticality of the epithelium.
TABLE 22.2 Histological and Cytological Differences among Major Classes of Lung Cancer
Type (Subtype)
Nucleus
Cytoplasm
Defining Feature(s)
Squamous
Chromatin coarse, clumped
Abundant
KP
Nucleoli often large and misshapen
Eosinophilic (red)
Intercellular bridges
Mitoses frequent
Epidermoid sheets
Fibrotic stromal response
SCLC
Fine granularity (salt and pepper)
Scant
Small cell size (<21 mm)
Nucleoli inconspicuous
Basophilic
Nuclear configuration
Mitoses very frequent
Nulear molding
Cell clusters
LCLC
Chromatin coarse, clumped
Abundant
Lack of differentiated features
Nucleoli prominent
Basophilic/amphophilic
Large cell size (>21 mm)
Mitoses frequent
Soid sheets and cell clusters
Carcinoid
Intermediate clumping
Intermediate abundance
Numerous neurosecretory granules
Nucleoli inconspicous
Granular
Ribbonlike cords or solid sheets
Mitotic rate <1/10 hpf
Basophilic/amphophilic
Spindle cell pattern
Nuclear consistency
Low mitotic rate
Atypical carcinoid
Intermediate clumping
Intermediate abundance
Neurosecretory granules
Nucleoli focally prominent
Granular
Ribbonlike cords or solid sheets
Mitotic rate 1-10/10 hpf
Basophilic/amphophilic
Intermediate mitotic rate
Necrosis
LCNEC
Intermediated to fine granularity
Abundant
Lack of differentiated features
Nucleoli inconspicuous
Basophilic/amphophilic
Large size (>21 mm)
Mitotic rate >1/10 hpf
Adenocarcinoma
Intermediate clumping
Abundant
Mucin vacuoles (>10% of cells)
Prominent nucleoli
Basophilic/amphophilic
Invasive glandlike nests and sheets
Mitoses frequent
Fibrotic stromal response
Bronchioloalveolar
Intermediate clumping
Abundant
Lepidic along alveolar septae
Prominent nucleoli
Basophilic/amphophilic
Mitoses usually infrequent
Several variants of squamous cell carcinoma are described, which may mimic other tumors either clinically or histologically. A papillary variant of squamous cell carcinoma, for example, may present as an exophytic endobronchial mass and histologically show a prominent in situ pattern. While an invasive component is usually present, a superficial biopsy may not be diagnostic of invasive tumor.
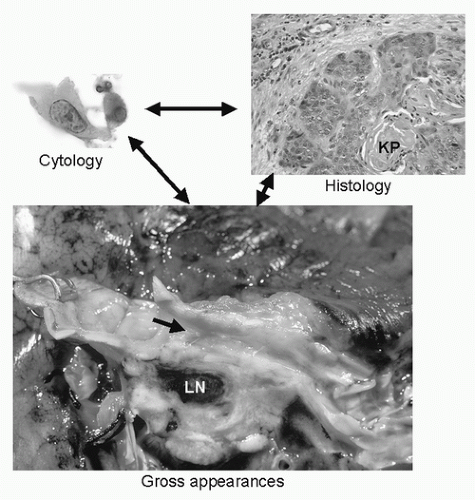
FIGURE 22.6 Various morphological appearances of squamous carcinoma. Cytological examination reveals bright orange, irregularly cells with conspicuous nucleolus. Histology of squamous cancers visible in both biopsy and resection specimens are characterized by irregular nests of cells, often with central KP. Early stage resected tumors are frequently ulcerated as indicated by the area of mucosal roughening and erythema (arrow). The ulcer overlies white invasive tumor tissue that surrounds a black anthrocotic LN. KL, keratin pearl; LN, lymph node. (See color plate.)
A small cell variant of squamous cell carcinoma may mimic neuroendocrine tumors including small cell carcinoma. Differences in nuclear pattern and mitotic activity are helpful in distinguishing these two tumors, as are neuroendocrine immunohistochemical stains. If sampled sufficiently, diagnostic squamous features (i.e., keratin, intercellular bridges) can be identified focally in basaloid squamous carcinomas.
Another consideration in the differential diagnosis is the distinction of squamous cell carcinoma from SCLC (discussed later). The nuclear architecture of squamous carcinoma uniquely contains large and atypical nucleoli that are not present in small cell carcinoma. There is also clumping of nuclear chromatin that permits distinction from the chromatin of SCLC.
Typically, squamous carcinomas spread directly through and replace tissue at the interface between normal lung and carcinoma. Squamous carcinomas can frequently be found spreading through the alveolar septae rather than along the surfaces of the alveolar walls as is typically observed in bronchioloalveolar carcinomas described later. However, a minority of tumors may also spread through the alveoli.
BRONCHIAL BIOPSIES AND THEIR PITFALLS
Endobronchial biopsy is the most commonly used procedure for obtaining a diagnosis in non-small cell carcinomas including squamous carcinoma and is described in detail elsewhere in this volume. In this procedure, a small fragment of bronchial mucosa is fixed in formalin and embedded in a block of paraffin wax for sectioning. Diagnostic tumor tissue my not be evenly distributed in the tissue and multiple sections of the block may be required to obtain a definitive histological result. Occasionally, squamous carcinomas may have an inaccessible endobronchial component and the easiest access to diagnostic material is through transbronchial biopsy. Here the same considerations of sampling artifact and representation of the tumor through all sections of the block are relevant.
Cytology Cytological specimens may be obtained through transbronchial or transthoracic fine-needle aspiration or through expectoration of sputum, either spontaneous or induced. Cytological specimens are fixed in alcohol-based fixatives and typically stained by the Papanicolaou method, which incorporates orange G dye that produces an intense waxy red-orange staining of squamous cell cytoplasm (Fig. 22.6).61 Elongated single cells (tadpole cells or fiber cells) are frequent. Nuclei are large, irregular shaped, and irregularly condensed. Less differentiated tumors contain sheets of cells with high nuclear/cytoplasmic (N/C) ratios with fewer differentiated squamous cells. Although sheets of cells with well-defined cell borders can be suggestive of squamous cell carcinoma, intercellular bridges cannot be easily visualized in cytological specimens and therefore are not a reliable criterion. The appearance of the aspirate can vary with the technique used to sample the tumor. In squamous cell carcinoma, for example, a sputum specimen will more likely sample better differentiated superficial tumor cells, whereas techniques such as bronchial brushing or fine-needle aspiration will sample more cells from within a tumor mass that may show more of the tumor sheets and less differentiated cells.61
The overall sensitivity and specificity of cytological specimens in a recent literature review of 16 studies by the Duke University Center for Clinical Health Policy Research were 0.66 and 0.99, respectively.62 The sensitivity of sputum specimens is highest for squamous cell carcinoma and small cell carcinoma (the centrally located tumors),62,63 and is most specific for squamous cell carcinoma.61 The diagnostic yield is better with larger tumors, which are centrally located, and in patients who present with bloody sputum.63
Differential Diagnosis A major differential diagnostic consideration in an endobronchial biopsy is the distinction between invasive squamous carcinoma and noninvasive squamous lesions in the respiratory mucosa. In some cases, in situ squamous carcinoma may exhibit considerable pleomorphism and may be difficult to distinguish from invasive carcinoma purely on the basis of the cytological appearances. An additional consideration is the extension of in situ tumor into the bronchial glands, which many mimic invasive carcinoma. Finally, the bronchial lining may respond to many different types of injury such as pneumonia, infarcts, and radiation or chemotherapy by converting from mucociliary epithelium to squamous epithelium that can mimic squamous cell carcinoma. It is therefore important that a history of these conditions accompany requests for pathological examination. In order to be completely confident of a diagnosis of invasive carcinoma, unequivocal invasion with nests of cells or single cell infiltrates eliciting a stromal response in the underlying mucosa is required.
The diagnosis of squamous carcinoma is usually made by conventional light microscopic examination of small biopsy or cytology specimens. Diagnosis can be difficult or misleading when small numbers of tumor cells are available for study and in approximately 30% of these small specimens, distinction of cell type cannot be made or the specimen is misdiagnosed. This can be a critical issue since agents such as the vascular endothelial growth factor (VEGF) blocker, bevacizimab,64 may cause cavitation in squamous tumors that can be life threatening while pemetrexed may be less effective against squamous tumors than against adenocarcinoma.65
DIAGNOSTIC IMMUNOHISTOCHEMISTRY OF INVASIVE SQUAMOUS CARCINOMA
Immunohistochemical markers may be used for diagnosis, prognosis, or prediction of response to treatment with targeted agents. In this section, the focus is mainly on the diagnosis whereas in the next, molecular lesions that are important in squamous carcinogenesis are discussed. Immunohistochemical predictors of response to targeted therapy are discussed elsewhere in this volume.
TABLE 22.3 Frequencies of Positive Diagnostic Immunohistochemistry Results by Histology
* Levels of expression as a function of the number of positive tumor cells for a specific marker.
−, <1%.
+, 1%-25%.
++, 25%-70%.
+++, >70.
Cytokeratin and Its Isotypes: Pan-CK, PCK5/6, CK7, and CK20 Immunohistochemical markers have been used in lung cancer largely to distinguish poorly differentiated metastatic tumors that may mimic the histological appearance of squamous carcinoma. Such tumors include large cell lymphoma, melanoma, germ cell malignancies, and sarcoma. The most helpful markers in this context are the cytokeratins (CKs). CK intermediate filaments are expressed in several different isotypic forms. Pan-CK antibodies recognize epitopes that are common to most of the CK isotypes. A pan-CK stain such as AE1/AE3 cocktail usually suffices to distinguish poorly differentiated squamous carcinomas from other poorly differentiated tumors. Occasionally, however, poorly differentiated tumors are pan-CK negative and these cases specific anti-CK isotypes such as CK5/6 may be positive and clarify the diagnosis.
A more complicated problem is the use of isotype-specific antikeratin antibodies to distinguish squamous carcinoma from other non-small cell lung carcinoma (NSCLC) types. With the emerging importance of squamous histology in predicting response to targeted agents, the question of whether immunohistochemical markers could be help to distinguish squamous from other non-small cell histologies has become more important. Several of the immunohistochemical markers useful for making this distinction are CKs (Table 22.3). The CKs form a large family of related proteins that associate to form mature filaments in epithelial cells and tumors.66,67,68 Central airway squamous tumors express different CKs than tumors originating from peripheral airways. Squamous carcinomas express CK5/6 at a frequency of >80%,69,70,71 but adenocarcinomas express this protein at a lesser frequency.70,71,72,73 However, there is so much overlap in the expression of CK5/6 among the tumor types, staining for CK5/6 by itself is not a reliable marker for squamous carcinoma.74
A second CK protein that has been suggested as a useful diagnostic aid is CK7. In squamous carcinoma, CK7 is notable by its absence with three quarters of squamous carcinomas negative for this marker.70,75,76,77 Here again, however, the number of positive cases found among squamous carcinoma is sufficient to limit the utility of the protein as a diagnostic discriminant of squamous carcinoma.
P63 P63 is a transcription factor and homologue of p53 that is important in epithelial cell differentiation. It is expressed by myoepithelial and reserve support cells and has been proposed as a possible marker of squamous phenotype. The marker is frequently expressed at high level in the nuclei of squamous carcinoma cells and overexpression is associated with p63 gene amplification.78 Several studies have shown that the marker has high sensitivity for squamous carcinoma with >95% of tumors immunoreactive with anti-p63 antibody.69,79,80,81 However, specificity is variable, with several studies reporting that 0% to 30% of adenocarcinomas express p63.79,80,81,82
Antibodies against p63 or CK5/6 or both have been paired with anti-thyroid transcription factor-1 (TTF-1) (discussed later) in a single immunohistochemical panel to distinguish squamous carcinoma from adenocarcinoma. Sensitivities and specificities for the double antibody test are high (80% to 100%) but the numbers of cases reported is small.82,83 Double antibody testing may ultimately prove useful for poorly differentiated tumors where little tissue is available but this test will require further validation in specific clinical contexts.
MOLECULAR PATHOLOGY OF SQUAMOUS CARCINOMA INCLUDING HIGH-THROUGHPUT GENE EXPRESSION ARRAYS
A variety of molecular abnormalities are present in squamous carcinoma that are not necessarily diagnostically useful but are part of the constellation of changes that accompany malignant transformation. Genetic changes in squamous tumors are numerous and can be grouped according to the molecular pathway they affect. Specific genetic lesions tend to group with specific histologies. To date, most mutations in squamous carcinoma are found to be associated with cell cycle genes and less frequently with tyrosine kinase pathway genes.84,85 A list of the most common genetic abnormalities and their frequencies in specific tumor types is presented in Table 22.4 and discussed in the context of specific tumor types.
TABLE 22.4 Frequent Genetic Changes in Lung Cancer: Approximate Prevalence of Mutations by Histology*
Functional Pathway
Gene
Chromosome
Genetic Lesion
SCLC
Sq Ca
Adeno
Cell cycle /apoptosis
TP53
17p13.1
Point mutation
70%
60%
40%
p16Ink4a
9p21
Deletion/methylation
<10%
60%
30%
rb1
13q14.2
Mutation/inactivation
90%
<10%
<10%
TK signaling
K-ras
12p12.1
Point mutation
<1%
<5%
30%
ErbB1 (EGFR)
7p12
Point mutation/in frame deletion
<5%
<1%
20%
*Adeno, adenocarcinoma; SCLC, small cell lung cancer; sq ca, squamous cell lung cancer; TK, tyrosine kinase.
Cell Cycle Genes Genes of the cell cycle were the first to be evaluated in lung cancer and are the most commonly mutated genes in squamous carcinoma.
TP53 TP53 is a multifunctional transcription factor that plays a complex role in a variety of processes including cell cycle regulation, DNA repair, and apoptosis. Of particular interest is its role as a cell cycle checkpoint in which TP53 interacts with DNA repair and recombination enzymes.86 This allows the cell to correct DNA damage during replication and the frequency of mutation and chromosomal rearrangement transmitted to daughter cells is thereby reduced. TP53 mutation interferes with DNA repair and may thus result in chromosomal instability, a major factor in malignant progression and resistance to chemotherapy. TP53 is the most commonly mutated gene in all lung carcinomas including squamous carcinoma.87 TP53 mutation does not appear to be associated with outcome in squamous carcinoma although it is associated with reduced survival in adenocarcinoma.88
CDKN2A (p16) P16 protein inhibits cyclin-dependent kinase 4 (CDK4) and inactivation of this inhibitor removes a brake on cell proliferation, enhancing tumor growth. P16 is one of the most frequently affected of the tumor suppressor genes and may be deleted89,90 or methylated91 in lung cancer. The gene is inactivated in approximately 60% squamous carcinoma.92 Methylation of p16 is an independent prognostic variable in NSCLC regardless of histological subtype.93 By contrast, in SCLC p16 is usually intact but the RB1 gene, also affecting progression through the cell cycle, is almost universally inactivated (see succeeding discussion of SCLC). Immunohistochemical tests assessing cell cycle-related proteins have been of more limited prognostic value. In one recent study, no single cell cycle protein (including p16) was of prognostic importance94,95 and only with combinations of markers could statistical significance be achieved.95 Prediction of outcome in individual tumors based on immunohistochemical testing of cycle proteins is unlikely to be accurate or reliable and it appears that only direct assessment of p16 gene methylation provides prognostic information.
Expression Microarrays other High-Throughput Technologies Until recently, biomarkers have been measured singly but oligonucleotide expression microarrays have permitted simultaneous evaluation of virtually all expressed genes in a single analysis. This technology has not yet found its way to broad clinical application but several important observations regarding lung tumors in general and squamous carcinoma in particular have been made utilizing this technology. First, microarray profiles strongly correlate with histology and clinical samples of squamous carcinoma can be distinguished from adenocarcinoma with a high degree of statistical certainty.56,96,97 Second, microarray data is reproducible98 and much of the variation in the reported literature can be attributed to differences in data interpretation that may be a complex exercise. Third, individual biomarkers are discoverable through application of microarrays and some of these markers may have clinical application. MAGE genes stand out in microarray experiments as some of the most highly overexpressed genes in central airway tumors including squamous carcinomas99 providing a target for ongoing immunotherapy trials.100,101 Fourth, it is possible to identify prognostically important subsets of genes102 that may predict response chemotherapeutic intervention103,104,105 or response to targeted agents.106 Whether gene expression profiles can be used to prospectively select appropriate therapy for individual patients is an important and to date unanswered question.
Additional high-throughput technologies are currently under investigation including proteomics107 and rapid largescale gene sequencing that will permit identification of all mutations within individual tumors (see succeeding discussion of adenocarcinoma). These technologies potentially could reach a level accuracy that will compel their use in the clinical management of squamous and other non-small cell carcinomas. However, they require accessing larger amounts of tumor for clinical study and changes in the way tissue is processed. These requirements could transform surgical tissue acquisition and pathology practices but will need careful validation and cost/benefit analysis before transfer from bench to bedside.
LARGE CELL LUNG CARCINOMA
Large cell lung carcinoma (LCLC) is an undifferentiated malignancy without features of small cell carcinoma, squamous cell carcinoma, or adenocarcinoma.60 Although the cell of origin of LCLC is not well defined, ultrastructural studies have revealed features of glandular or squamous differentiation that cannot be appreciated by light microscopy. LCLC thus represents an extremely poorly differentiated NSCLC without histological features that permit ready assignment to one of the more usual and better-differentiated forms of lung carcinoma. With loss of differentiating features comes extremely aggressive biological behavior. These tumors comprise approximately 9% of primary lung malignancies.108
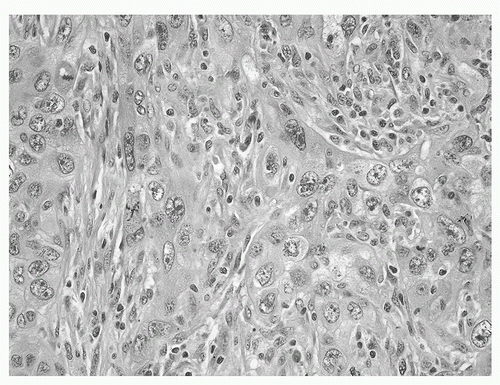
Histology of Large Cell Lung Carcinoma LCLCs are composed of poorly differentiated large cells (>21 microns) with prominent nucleoli and abundant, clearly visible cytoplasm (Fig. 22.7). Cells and nuclei are usually separate and discrete and less prone to deformation than the cells of small cell carcinoma. Tumor cells are generally arranged in nests or sheets. Nuclei are large and N/C ratios may be high. Mitoses are numerous and areas of necrosis are common.
The category of LCLC is heterogeneous and several variants of this tumor type have been described based on histology and immunohistochemical properties. These include clear cell carcinoma, large cell carcinoma with rhabdoid phenotype (rhabdoid carcinoma), and lymphoepithelioma-like carcinoma as well as two variants discussed elsewhere in this chapter, basaloid carcinoma and large cell neuroendocrine carcinoma (LCNEC). Clear cell carcinoma and rhabdoid carcinoma are terms that convey the essential cytological appearances of these neoplasms. The rhabdoid type has a particularly poor prognosis.109,110,111,112
The lymphoepithelioma-like variant resembles the lymphoepithelial carcinoma seen in the nasopharynx (undifferentiated epithelial cells with an intermixed prominent lymphoid infiltrate); this rare variant that affects young, Asian, nonsmokers113,114 is associated with Epstein-Barr virus (EBV). These tumors are Bcl-2 positive by immunohistochemistry (IHC) and express EBER-1 by in situ hybridization,114 suggesting viral etiology. Surgery is the treatment for early stage tumors, while multimodality treatment is used in advanced cases. Although quick to metastasize, this variant shows a favorable response to chemotherapy.114,115,116,117,118
FIGURE 22.7 Large cell undifferentiated lung carcinoma exhibits no differentiating features and is composed of large cells with coarsely clumped nuclei and prominent nucleoli. Mitoses are abundant. (See color plate.)
Cytology Because the diagnosis of large cell carcinoma is made after the exclusion of squamous, glandular, or small cell components, it is often classified as a non-small cell carcinoma on small tissue specimens such as transbronchial biopsies and cytological specimens. Cytological smears show an undifferentiated carcinoma without squamous, glandular, or small cell features. Smears are usually cellular and composed of both single cells and syncytial aggregates. Cells are large with high N/C ratios, large nuclei with prominent or multiple nucleoli in a background of necrosis.
Immunohistochemistry of Large Cell Lung Carcinoma The immunohistochemical staining properties of LCLC are listed in Table 22.3. In general, they are similar to other forms of NSCLC with the exception of a higher level of expression of proliferation markers, reflecting the rapid growth of these tumors.
UNCOMMON BUT SIGNIFICANT VARIANTS OF NON-SMALL CELL LUNG CARCINOMA
Several histological variants of NSCLC are significant because of their distinct morphology and prognosis. The most prominent among these variants are basaloid carcinoma and pleomorphic carcinoma.
Basaloid Carcinoma This variant histology may be found admixed with other forms of non-small cell carcinoma or as the sole cell type in a subgroup of lung carcinomas. Basaloid histological features include lobular growth of relatively small cells with dense nuclei, inconspicuous nucleoli, scant cytoplasm, a high mitotic rate, and peripheral palisading.119 Misinterpretation of these tumors as SCLC has been described in fine-needle aspirations.120,121 Small cell variant of squamous carcinoma is also distinguished from undifferentiated small cell carcinoma by nuclear features including prominent nucleoli and a coarse clumping of the chromatin. In doubtful cases, immunohistochemical stains for neuroendocrine markers may be applied (see succeeding discussion).
The reported frequency is about 6% of all lung cancers.119 The reported prognostic significance of basaloid histology has been inconsistent with one study finding reduced actuarial 5-year survival for basaloid tumors in comparison to poorly differentiated squamous tumors122 but a second similar-sized study finding similar survival for the two tumor types.123 Since these tumors are rare, additional studies, perhaps through a multicenter registry, will be necessary to better characterize their behavior.
Carcinomas with Pleomorphic, Sarcomatoid, or Sarcomatous Elements These carcinomas have been recognized under various names for many years including spindle cell carcinoma, giant cell carcinoma, pleomorphic carcinoma, and carcinosarcoma. This category consists of tumors that are composed exclusively of sarcoma or pleomorphic tumor cells or of tumors that contain a component of sarcomatoid or pleomorphic cells along with tumor of a more usual histological type. In the most recent WHO classification,1 these tumors are grouped in a single diagnostic category. These tumors are uncommon and usually reported as single cases but two larger series have also been published.124,125 The median survival in these series is 10 months.
Sarcomatoid tumor histology is characterized by the presence of spindle areas that resemble sarcoma.124,125 The sarcomatous element in this variant type may contain muscle, bone, or cartilage as well as undifferentiated spindle cells.124,125 There also may be mixtures of epithelial tumor and sarcomatous components, referred to as carcinosarcoma. The giant cell variant of the category consists of highly pleomorphic cells that form multinucleated giant cells, usually accompanied by a heavy inflammatory infiltrate. In most cases, these tumors have biomarker profiles similar to those of other lung tumors, expressing CK7 and TTF-1.125 However, in approximately 25%, either one or the other or both of these biomarkers is (are) absent and these negative tumors tend to be those with the most sarcomatous histological appearance.
The biological significance of this category of tumor has been emphasized by the recent description of the stromal molecular and cellular properties in tumors that are otherwise considered epithelial. This pattern of differentiation has been referred to as epithelial mesenchymal transition (EMT). Properties associated with EMT include change in cell culture characteristics from the sheetlike pattern of epithelial cells to a more single cell infiltrative stromal pattern of growth.126 This morphological change is accompanied by increased expression of vimentin intermediate filament and the transcription factor ZEB1 and by reduced expression of the adhesion molecule E-cadherin, the transcription factor SNAIL, and EGFR.127 Such molecular changes are most evident in tumors that exhibit elements of sarcomatoid differentiation but poorly differentiated tumors without sarcomatous elements may also lose expression of E-cadherin. Loss of E-cadherin imparts a poor prognosis independent of stage128 and resistance to EGFR blockade.77,106,127,129,130,131 It seems likely that the loss of E-cadherin represents part of a continuum of dedifferentiation that at its most extreme is reflected in the pleomorphic tumor category. This category will require unique therapeutic consideration, especially as targeted drugs become increasingly available for tumors with specific molecular phenotypes.
SMALL CELL LUNG CARCINOMA
The separate and unique histological features of SCLC were first recognized in 1926 by Bernard who introduced the tumor as oat cell sarcoma.132 This subcategory took on greater importance when it was shown that the response to chemotherapy in these tumors differed substantially from the response of other tumor types with the SCLC being particularly sensitive to mitotic inhibitors.133 It is for this reason that the main dichotomy of clinical relevance in lung cancer pathological diagnosis remains the distinction between SCLC and all other forms of lung carcinoma (NSCLC).
Histology of Small Cell Lung Carcinoma SCLC is an invasive carcinoma composed of small (<21 microns or <3 lymphocyte diameters) cells with scanty cytoplasm (Fig. 22.8). Histologically, these tumors are distinguished by their finely granular nuclei (salt and pepper chromatin), by their small and relatively inconspicuous nucleoli, and by the tendency for the nuclei to become easily deformed by contact with other cells and other structures (nuclear molding). These tumors are highly proliferative and rarely is the mitotic rate less than 10 mitoses per 10 high-power fields (hpf) so that virtually every hpf contains one or more mitoses. The neoplastic cells in this tumor type are fragile, and crush artifact is common particularly in small biopsy samples. Lymphocytes and other inflammatory cells can also undergo crush artifact and it is therefore of some importance that definitive diagnosis be based on examination of well-preserved cells where nuclei are clearly visible. A unique feature of SCLC is the Azzopardi effect consisting of an accumulation of chromatin in the vascular walls supplying the tumor. In a great majority of cases, the diagnosis of SCLC is obvious by histological examination alone. However, in some cases, immunohistochemical studies can serve to buttress the diagnosis and provide confirmation of diagnosis.
Within the category of SCLC, there is considerable variation in cell size and cellular configuration. For several years, subsets of SCLC were included in the SCLC category. The 1967 WHO classification included oat cell carcinoma and an intermediate cell variant that differed from classical oat cell carcinoma in cell size and amount of cytoplasm. These categories proved to be of no prognostic significance and the two categories were combined in the latest classification into a single small cell category. This tumor type comprises 15% to 20% of all lung cancers but its frequency may be decreasing.59,134 Typically, small cell carcinomas present as an endophytic lesion in a central bronchus with mediastinal lymph node (LN) metastases.
FIGURE 22.8 SCLC as found on cytology, histology, and IHC. On the upper left are clusters of small cells with scant cytoplasm, nuclear molding (arrow), and finely granular nuclei with inconspicuous nucleoli. Macrophage (Mac) provides size comparison. The frame on the upper right shows the histology of SCLC with closely packed cells with scanting cytoplasm with streaming nuclei. NCAM and TTF-1 stains are strongly positive along plasma membranes and in the nuclei. Mac, macrophage; NCAM, neural cell adhesion molecule; TTF-1, thyroid transcription factor-1. (See color plate.)
Cytology Success in identifying SCLC by cytological examination is partially dependent on the type of specimen available for examination. SCLC may be readily identified bronchial washings and brushings where the cells are well preserved and in these cases, cytology may be crucial in arriving at a definitive diagnosis. However, SCLC has been infrequently identified in screening trials135,136 in part because SCLC is not well preserved in expectorated sputum and also perhaps because the disaggregation process may damage the fragile cell of SCLC. The cytological features of SCLC correspond to what is seen in well-preserved tissue sections. Single cells or small clusters of cells less than 21 microns in diameter have a high N/C ratio with only a thin sometimes barely visible rim of cytoplasm around and enlarged nucleus (Fig. 22.8). Nuclear fragmentation is often present in association with better-preserved cells. The nucleus again has finely granular (salt and pepper) chromatin and small, inconspicuous nuclei. In small clusters of cells, nuclei are often molded against one another. Nuclear features are crucial and excellent preservation of cells is required for diagnosis. Cells that may resemble SCLC are basilar cells of the respiratory mucosa that usually are smaller and more uniform that the cells of SCLC. Lymphocytes may also cause confusion but usually only in poorly preserved specimens.
Diagnostic Immunohistochemisty of Small Cell Lung Carcinoma Immunohistochemical stains can be used to verify the neuroendocrine nature of the tumor or help distinguish SCLC from other NSCLC (Fig. 22.8). SCLC almost always expresses CK but the amount of this intermediate filament may be quite small, particularly in less than that optimally preserved specimens. CK expression serves to distinguish SCLC from other small blue cell tumors such as lymphoma, which occasionally can mimic SCLC. SCLC, like adenocarcinomas of the lung (see succeeding discussion), is usually positive for the primitive lung differentiation gene TTF-1 with several studies documenting expression rate in at least 85% of these tumors.71,137,138,139,140,141,142,143,144 In specific contexts, TTF-1 may be useful in distinguishing SCLC from small cell tumors of other sites. For example, while this marker is expressed in a large percentage of SCLC, histologically similar Merkel cell tumor of dermal origin and small cell carcinoma of ovary are virtually always negative for this marker.140,141,142,144,145,146 Small cell cervical and colon carcinomas are occasionally positive (10% to 15%140,146,147) but up to 50% of transitional carcinomas of bladder140,147,148,149 and over 70% of esophageal small cell tumors are reported positive.150 Reported results for small cell prostate carcinomas have been variable with some studies indicating high frequency of expression147 and other low frequency of expression.140,151 The utility of TTF-1 in distinguishing site of origin of unknown primary is therefore highly context dependent.
A distinguishing feature of SCLC is its expression of neuroendocrine markers including neuron specific enolase, synaptophysin, neural cell adhesion molecule (NCAM) (CD56), and Leu-7 (CD57).152,153,154 Approximately 50% of SCLCs also express chromogranin A in sufficient quantity to be detectable in conventional immunohistochemical tests so that in doubtful cases a negative chromogranin is uninformative. The quantity of chromogranin in SCLC is usually less than that present in carcinoid, so that in cases with strongly positive chromogranin stains carcinoid tumor should be excluded. A salient feature of SCLC is its high growth fraction; as determined by Ki-67 labeling procedures, the growth fraction usually exceeds 50%. Ki-67 may be helpful in distinguishing SCLC from other neuroendocrine tumors of the lung. A negative differentiating marker is EGFR, which is expressed in NSCLC but not in SCLC.154 Finally, it has been reported that c-kit receptor (CD117) is nearly always expressed by high-grade neuroendocrine carcinomas including SCLC and LCNEC,155,156,157,158 an observation that has been fully exploited neither diagnostically nor therapeutically. The expression of CD117 is apparently not associated with mutation of the c-kit receptor gene159 and no relationship to survival or response to chemotherapy has been shown to date.160
The application of immunohistochemical staining procedures to lung tumors has revealed considerable overlap in staining properties. It is known for example that about 20% of adenocarcinomas are focally positive for NCAM, a molecule that otherwise is almost universally expressed by SCLC. This suggests a degree of phenotypic plasticity in lung tumors that is confirmed in gene profiling studies (see discussion that follows).
Molecular Pathology in Small Cell Lung Carcinoma The unique histological and immunohistochemical features of this tumor are a reflection of underlying genetic changes that are increasingly better defined. SCLC was among the first of the lung tumor types in which genetic changes were defined. These changes included structural chromosomal abnormalities (deletion [3p(14-23)161] and the mutations described and listed in Table 22.4. The pathways most frequently affected by mutation involve cell regulation and tyrosine kinase signaling genes including KRAS84,162 and EGFR84,163 are rarely mutated. In the succeeding discussion, genetic lesions are grouped by pathway as in the previous discussion of squamous carcinoma.
Cell Cycle Genes A number of the mutations and chromosomal rearrangements that affect cell cycle genes are present in SCLC.
RB1/CDKN2A (p16)RB1 was first identified as a tumor suppressor gene in retinoblastoma. Knudson’s “two-hit” model of carcinogenesis, whereby a dominant tumor suppressor gene is inactivated by two mutational events eliciting tumor formation, was formulated in 1971 to explain retinoblastoma tumorigenesis.164 Fifteen years later, the retinoblastoma gene, RB1, was cloned165 and the relevance of RB1 to lung cancer was demonstrated.
RB1 encodes a phosphoprotein that binds to the transcription factor E2F. Phosphorylation of RB1 releases E2F and transition from the G1 to S phase of the mitotic cycle occurs. RB1 is therefore an important cell cycle regulator and tumor suppressor gene. Loss of RB1 results in an increase in cell proliferation and more rapid tumor growth.
Structural changes in the RB1 gene in SCLC lines and tumors have been reported and complete absence of RB1 protein has been reported to affect all SCLC.166,167,168 The mechanism of RB1 inactivation in human tumors is still not completely understood. Although RB protein is absent in SCLC, DNA sequencing has identified mutations in only a minority of tumors and these consist primarily of deletions resulting in frame shifts or stop codons.169
The mutational pattern evident in cell cycle genes in SCLC is distinct from that in NSCLC with the latter frequently affected by loss of p16 with and overexpression of cyclin D1 rather than the near universal loss of RB1168 observed in SCLC.
TP53 TP53 is more frequently mutated in SCLC than in the other non-small cell forms of lung cancer. Loss of TP53 function with associated loss of cell cycle checkpoint function and impairment of apoptotic pathways undoubtedly contributes to the aggressive growth and hypermutability that are features of this tumor.
Gene Expression Profiles In virtually all the nucleotide microarray analyses, small cell tumors emerge as a separate phenotypic category with numerous gene expression difference with the non-small cell tumors.170 Available microarray data for SCLC has considerably expanded the number of potential biomarkers that may be useful in the differential diagnosis and detection of SCLC. Moreover, these studies have indicated that many of the genes expressed in SCLC are also found during lung differentiation (see succeeding discussions).
To date, however, the molecular features of SCLC have not been sufficiently definitive nor have they added sufficient independent information to histological diagnosis to justify the general application of diagnostic molecular testing in this tumor. The diagnosis of this neoplasm therefore continues to rest on histological examination supplemented by immunohistochemical studies in difficult cases.
MIXED SMALL CELL AND NON-SMALL CELL CARCINOMA
It is of interest that a large proportion of small cell carcinomas contain a component of non-small cell tumor. These tumors include large cell carcinoma, adenocarcinoma, and squamous carcinoma. In a recent review of 100 small cell carcinomas, Nicholson et al.171 found 72 pure small cell carcinomas and 28 combined small cell carcinomas. Sixteen cases were combined with large cell carcinoma, nine with adenocarcinoma, and three with squamous cell carcinoma.
BRONCHIAL CARCINOID, ATYPICAL CARCINOID AND LARGE CELL NEUROENDOCRINE CARCINOMA
The term carcinoid was originally coined in 1907 to describe a subset of gastrointestinal epithelial tumors that were less aggressive than the conventional gastrointestinal carcinoma and were therefore designated carcinoid tumors rather than carcinoma.172 It was subsequently demonstrated that similar tumors existed in the lower respiratory tract.173 Currently, these tumors together with SCLC and LCNEC are regarded as neuroendocrine and are considered part of a continuum. Carcinoid tumor is the lowest grade and least aggressive of this group and SCLC is the highest grade and most aggressive.174,175 This category also includes atypical carcinoid, which characteristically has an elevated mitotic rate in comparison to typical carcinoid and behaves more aggressively with a metastatic rate of approximately 50%. Finally, LCNEC is an aggressive, high-grade tumor that was first described in 1991175 as an undifferentiated tumor that is intermediate in morphological features and prognosis between atypical carcinoid and SCLC.
Typical Carcinoid Tumor Typical carcinoid tumors may arise in the either central or peripheral airways. They usually have strikingly different macroscopic features in the two locations. The central airway tumors are relatively large (mean diameter 3 cm)176 and grow as endobronchial masses that may obstruct the large bronchi (Fig. 22.9). The secretory products of these tumors also may induce swelling of adjacent tissues that augments the obstruction caused by the tumor itself. These tumors may extend into the bronchial wall but such infiltration does not necessarily imply aggressive growth and is not a criterion for atypical carcinoid. The sectioned surface of carcinoid tumor is usually gray and homogeneous. The histological features that distinguish carcinoid tumors from NSCLC are relative uniformity of the tumors cells, abundant grayish granular cytoplasm, lack of tumor cell necrosis, and round to oval nuclei with finely granular (salt and pepper) nuclear chromatin and inconspicuous nucleoli. Carcinoid cells form small clusters without true gland formation in a pattern that is variously described as organoid or insular. Cells and nuclei are frequently oriented perpendicularly to the basement membrane, forming palisading or rosettelike patterns. To distinguish slow-growing typical carcinoids from more aggressive tumors, the diagnosis is limited to those tumors with <2 mitoses per 2 mm2 (<10 hpf) and no necrosis.60
Only gold members can continue reading. Log In or Register to continue