Aspirin monotherapy represents a standard therapy for preserving patency after coronary artery bypass grafting. Randomized trials addressing whether dual antiplatelet therapy is superior to single antiplatelet therapy to achieve graft patency early after coronary surgery have shown inconsistent results. We performed a meta-analysis of randomized controlled trials comparing single versus dual antiplatelet therapy after coronary artery bypass grafting. In a systematic published works search, 5 randomized controlled trials meeting inclusion criteria were identified. Pooled efficacy and safety data were abstracted and analyzed using a fixed-effects model. The 5 trials included 958 patients and a total of 2,919 grafts with treatment up to 1 year after coronary bypass surgery. Early occlusion was identified in 165 (6.5%) of 2,526 bypass grafts. Early occlusion occurred in a greater proportion of grafts among patients treated with single therapy (105 of 1,369; 7.7%) compared with dual antiplatelet therapy (69 of 1,386; 5.0%; p = 0.005). The odds ratio for graft occlusion with single versus dual therapy was 1.59 (95% confidence interval 1.16 to 2.17). For vein grafts, single antiplatelet therapy was associated with a significantly increased graft loss rate (91 of 846; 10.8%) versus dual antiplatelet therapy (57 of 860; 6.6%; odds ratio 1.70 [1.20 to 2.40]; p = 0.003). There was no effect on arterial graft patency. Bleeding was noted in 3.3% and 4.9% of single and dual therapy treated patients, respectively, with only 3 trials reporting bleeding outcomes. In conclusion, among 958 patients randomly assigned to either single or dual antiplatelet therapy for up to 1 year after coronary bypass surgery, single antiplatelet therapy significantly increased the risk for graft occlusion, an effect isolated to vein grafts, not arterial grafts.
Patients undergoing coronary artery surgery routinely receive aspirin therapy, as a standard treatment for preserving bypass graft patency. However, despite this therapeutic approach, early graft loss due to thrombosis remains a concern. Previous studies using combined antithrombotic approaches with aspirin and warfarin failed to show a benefit of the addition of warfarin over aspirin alone. In coronary arterial disease in prothrombotic conditions, such as after coronary stent implantation, more intensive antiplatelet treatments using dual antiplatelet therapy reduce the incidence of abrupt stent thrombosis. A similar approach may provide benefit to increase the patency rate of coronary bypass grafts. We performed a systematic review and quantitative meta-analysis of randomized clinical trials of mono- and dual antiplatelet therapies combining aspirin and thienopyridine antagonists (clopidogrel) to assess the potential benefits and risks of this approach.
Methods
We carried out a comprehensive published works search of PubMed ( http://www.ncbi.nlm.nih.gov/pubmed ). The following keywords were used in the search: (“Aspirin and Clopidogrel” and “Coronary Artery Bypass” and “Graft Patency”). The search also included review of bibliographies of selected studies. To be eligible for this study, the deadline for publication was March 2013. No unpublished trials were included.
Studies included in the analysis had to meet all of the flowing criteria: (1) randomized clinical trial evaluating single versus dual antiplatelet therapy for ≥30 days, (2) prespecified end point of graft patency assessed by angiographic methods in all subjects, and (3) data reported per coronary bypass graft. Nonrandomized trials were excluded. Non-English language publications were also excluded. Five studies were identified that compared monotherapy with dual therapy. Four studies compared aspirin versus aspirin plus clopidogrel; 1 study compared clopidogrel with aspirin plus clopidogrel.
The data extracted from the eligible studies included: first author, year of publication, study design, sample size, average patient age, graft type, treatment, method of assessment, clinical outcome (percentage of graft patency and graft occlusion), and safety assessment (bleeding). Studies were assessed for quality in the following 3 areas: randomization, reporting of withdrawals, and generation of random numbers. Data extraction was preformed independently by 2 reviewers (AJT and AGN). Any disagreements between the reviewers were discussed to achieve a consensus.
The primary outcome of this meta-analysis is overall graft patency, comparing single versus dual antiplatelet therapy. Secondary outcomes included safety assessments.
Statistical analysis was performed using MetaEasy 2007, London, England. Odds ratio (OR) and 95% confidence intervals (CIs) were used as summary statistics. Contingency tables were constructed from abstracted data from the 5 individual studies. Trial heterogeneity was assessed with Cochrane’s Q. A summary OR and 95% CI were calculated using a fixed-effects model, as there was no evidence of trial heterogeneity. A 2-sided p value <0.05 was considered statistically significant. In cases of statistical significance, the number needed to treat and absolute risk difference were also calculated.
Results
Table 1 lists the characteristics of the 5 randomized trials included in this analysis. A total of 958 patients were randomly assigned to receive either mono- or dual antiplatelet therapy. All studies enrolled patients who were aged ≥59 years, with most being men (85%). A total of 878 patients completed the follow-up assessments, ranging from 30 days to 12 months after coronary bypass surgery. Four of the studies used multidetector computed tomography angiography and 1 study used invasive angiography to assess graft patency.
| Study | Patients | Age (Yrs) | Men | Treatment | Method of Assessment | Primary End Point | Safety Assessment | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mono | Dual | Monotherapy | Dual Therapy | Monotherapy (%) | Dual Therapy (%) | Monotherapy | Dual Therapy | ||||
| Gao et al | 102 | 95 | 62.4 ± 9.9 | 60.5 ± 10.1 | 83 | 83 | Clopidogrel | ASA + clopidogrel | Cardiac CT | Graft patency at 12 mo | None |
| Gao et al | 125 | 124 | 59.8 ± 7.9 | 57.9 ± 8.3 | 84 | 82 | ASA | ASA + clopidogrel | Cardiac CT | Graft patency at 3 mo | None |
| Kulik et al | 57 | 56 | 68.1 ± 7.4 | 64.9 ± 7.5 | 88 | 91 | ASA | ASA + clopidogrel | Intravascular ultrasound and coronary angiographies | SVG intimal hyperplasia | Bleeding and cardiovascular events |
| Sun et al | 50 | 49 | 63.5 ± 8.1 | 65 ± 9.6 | 95 | 98 | ASA | ASA + clopidogrel | Cardiac CT | Graft patency at 30 days | Bleeding and cardiovascular events |
| Mannacio et al | 150 | 150 | 58.9 ± 8.3 | 59.4 ± 7.7 | 75 | 730 | ASA | ASA + clopidogrel | Cardiac CT | Graft patency at 12 mo | Bleeding and cardiovascular events |
A total of 2,919 grafts were examined among the 5 studies, 1,369 grafts in the monotherapy group and 1,386 grafts in the dual therapy group. As listed in Table 2 , the mean graft patency was 92.3% (1,264 of 1,369) in the monotherapy group and 95.0% (1,317 of 1,386) in the dual therapy group for an absolute risk difference of 2.7% and a number needed to treat of 37 (chi-square p = 0.005). The mean graft occlusion was 7.7% (105 of 1,369) in the monotherapy group and 5.0% (69 of 1,386) in the dual therapy group. In pooled analysis, the summary OR of graft occlusion in the monotherapy group compared with that in the dual therapy group was 1.59 (95% CI 1.16 to 2.17).
| Study | No. of Patients Assessed | Grafts | ||||||
|---|---|---|---|---|---|---|---|---|
| Monotherapy | Dual Therapy | |||||||
| Monotherapy | Dual Therapy | Total Grafts | Venous Grafts | Arterial Grafts | Total Grafts | Venous Grafts | Arterial Grafts | |
| Gao et al | 102 | 95 | 252/13 | 154/10 | 98/3 | 253/8 | 163/6 | 90/2 |
| Gao et al | 111 | 113 | 340/35 | 231/33 | 109/2 | 353/23 | 239/20 | 114/3 |
| Kulik et al | 45 | 45 | 156/7 | 104/7 | 52/0 | 166/8 | 108/6 | 58/2 |
| Sun et al | 39 | 40 | 154/11 | 88/6 | 66/5 | 159/8 | 93/6 | 66/2 |
| Mannacio | 144 | 144 | 467/39 | 267/35 | 200/4 | 619/22 | 257/19 | 362/3 |
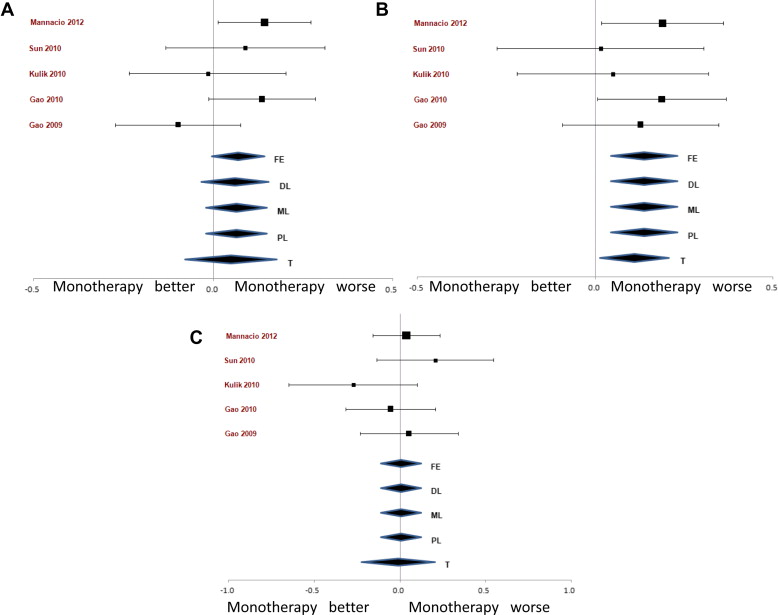
The treatment effects among venous and arterial bypass grafts were analyzed separately ( Figure 1 ). Among venous grafts, 844 were evaluated within the monotherapy group and 860 within the dual therapy group, for a total of 1,706 grafts. The mean graft patency was 89.2% (753 of 844) in the monotherapy group and 93.4% (803 of 860) in the dual therapy group. The occlusion rate of 10.8% (91 of 846) in the monotherapy group and 6.6% (57 of 860) in the dual therapy group led to an absolute risk difference of 4.2% and a number needed to treat of 24 (chi-square p = 0.003). The OR of venous graft occlusion in the monotherapy group compared with that in the dual therapy group was 1.70 (95% CI 1.20 to 2.40).