Mesothelial and Other Less Common Cysts of the Mediastinum
Gaetano Rocco
Thomas W. Shields
In addition to the previously described enterogenous and neuroenteric cysts (Chapters 201, 202 and 203), other mediastinal cysts include mesothelial (pleural, pericardial) thoracic duct, thymic, parathyroid, and hydatid cysts. Cystic lesions arising in the mediastinum are most commonly located in the anterior and visceral compartments. Pathologic features of these cysts, as expected, are related to their tissue of origin. Despite their rarity and the paucity of symptoms associated with their presence in most cases, a clear knowledge of etiology, pathology, and clinical significance of each variety is necessary.
Mesothelial Cysts
Mesothelial cysts comprise a variety of cysts that have been reported as pleuropericardial cysts, pleural cysts, lymphogenous cysts, and simple mesothelial cysts of the mediastinum. These are essentially unilocular cysts filled with clear or slightly yellowish thin fluid. Most often they are incidental radiologic findings. They may be classified as one of two types: (a) pleuropericardial cysts and (b) other mesothelial (pleural) cysts. Mesothelial cysts are estimated to occur in approximately 1 of every 100,000 persons. Ochsner and Ochsner,73 in reporting 42 cases of various congenital cysts of the mediastinum, noted that 14 (33%) were mesothelial in type; of these, 11 were pleuropericardial and 3 were “pleural” in location. More recently, Takeda and associates103 found that 18% of 105 mediastinal cystic lesions were mesothelial cysts. Stoller and associates101 reported likewise that the right cardiophrenic angle was most often involved; 50% to 70% of these cysts were located in the right cardiophrenic angle (Fig. 204-1), 20% to 30% in the left (Fig. 204-2), and the remainder elsewhere in the visceral compartment. In light of their prevalence at the cardiophrenic angle, appreciation of the anatomy of the anterior cardiophrenic angle is important in making an accurate diagnosis. The anterior cardiophrenic angle,96 is the space bounded by the pericardium medially, the chest wall anteriorly, the pleura laterally, the phrenic nerve posteriorly, and the diaphragm inferiorly. A multiplicity of lesions can be noted in this area; accurate diagnosis is essential. The most important lesion with regard to differential diagnosis is a foramen of Morgagni hernia, which can contain visceral structures and be associated with serious consequences (see Chapter 54). Other important lesions include ventricular aneurysms, mediastinal tumors, enlarged pericardial fat pad, diaphragmatic tumors, diaphragmatic eventration, and pulmonic or pleural processes.
Pleuropericardial Cysts
Pickhardt82 is responsible for the first surgical resection of a pleuropericardial cyst from the mediastinum. According to the review by Lillie and associates,58 cystic lesions surrounding the heart had been described as early as 1854. One of the more intriguing aspects of pericardial cysts is their origin. Lambert53 was the first to discuss the cause of pericardial cysts. He stated that the pericardium arises from a series of disconnected lacunae early in embryonic life. As the embryo enlarges, these lacunae merge to form the pericardial coelom. Failure of one of these lacunae to merge results in subsequent cyst formation.
Further evaluation of the development of the pericardium revealed the presence of ventral and dorsal parietal recesses during embryonic development (Fig. 204-3). The ventral parietal recess is a diverticular structure where the majority of pericardial cysts are located. Lillie and associates58 maintained that pericardial cysts form secondary to persistence of the ventral parietal recess. Constriction of the diverticular neck of the recess or complete obliteration of the neck results in a mesothelium-lined cyst. This is believed to explain the frequency of pericardial cysts located at the cardiophrenic angle. Of 37 cases of mesothelial cysts reviewed by Lillie and colleagues,58 17 were located at the cardiophrenic angle, especially on the right side. Indeed, in the series of 18 pleuropericardial cysts reported by Kutlay and associates,52 11 cysts were located in the right cardiophrenic angle (61%), 4 in the left angle (22%), and 3 in other locations (16%). The latter 3 cysts were in the right paratracheal area immediately above the heart. Cysts located outside this area are believed to occur secondary to complete obliteration of the diverticular neck and subsequent translocation during embryonic growth (Table 204-1). The few pericardial cysts that occur outside of the anterior cardiophrenic angle (8% to 16%) are usually superior to the heart but again seem to be more often located on the right side rather than the left (Fig. 204-4). A frequent site is between the superior vena cava and the azygos vein adjacent to the wall of the trachea. Stoller and associates101 were among the first investigators
to note that other pericardial cysts could also be located in association with either hilar area or in the neighborhood of the aortic arch. Any of these cysts may have an open communication into the pericardium. A solid tissue pedicle may run to or toward the pericardium, or the cyst may be free of any such attachment to the pericardium.
to note that other pericardial cysts could also be located in association with either hilar area or in the neighborhood of the aortic arch. Any of these cysts may have an open communication into the pericardium. A solid tissue pedicle may run to or toward the pericardium, or the cyst may be free of any such attachment to the pericardium.
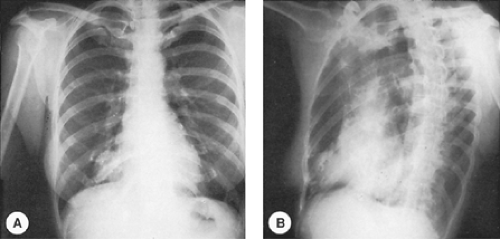 Figure 204-1. A,B: Posteroanterior and oblique radiographs of the chest reveal the presence of a pleuropericardial cyst in the right anterior cardiophrenic angle. |
Both Lambert53 and Lillie and colleagues58 reported that, pathologically, these cysts are lined with mesothelium and contain a clear water-like fluid. Hence these lesions were initially named spring water cysts. Le Roux56 noted that most commonly, these cysts are unilocular and that 5% of pericardial cysts communicate with the pericardium through definable tube-like structures. When communication of the cyst with the pericardium persists, the lesion may be considered a pericardial diverticulum (Fig. 204-5).
Le Roux and colleagues stated that only 20% of pericardial cysts present symptomatically, usually with dyspnea or chest wall discomfort. It is an interesting observation that symptoms rarely dissipate with excision unless the cyst was of significant size. The possibility of an acute hemorrhage into the cyst occurring, with resulting tamponade, has been described both in the adult and in pediatric patients by several authors.12,104 This can be corrected with resection of the cyst by either a median sternotomy or a video-assisted thoracic surgical technique (VATS).12,104 In addition, partial erosion of the right ventricle and of the superior vena cava has been reported by Chopra16 and Mastroroberto61 and their colleagues, respectively.
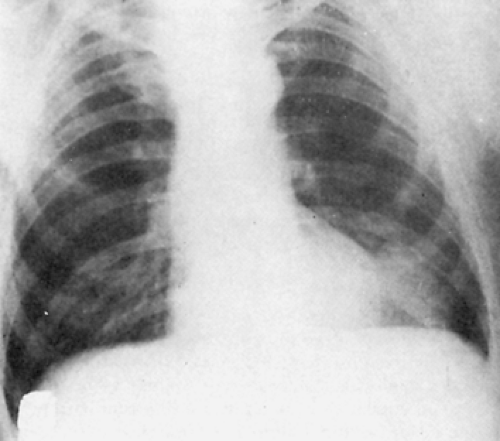 Figure 204-2. Posteroanterior view of chest radiograph reveals the presence of a left-sided pleuropericardial cyst. |
Radiography of the chest, echocardiography, and chest computed tomography (CT) scanning are the most commonly used modalities for diagnosis of pericardial cyst. On infrequent occasion, contrast studies of the gastrointestinal tract are necessary to rule out a foramen of Morgagni hernia, but CT examination often reveals bowel in the mass when the lesion is a foramen
of Morgagni hernia (Fig. 204-6). Pineda and colleagues have emphasized the distinctive ability of current cross-sectional imaging techniques to delineate masses at the cardiophrenic angle83 and suggest that such masses should be interpreted as soft tissue components predictive of malignancy.83 Pugatch,87 Kaimal41 and, more recently, Kim and associates44 have described the essential CT features of pericardial cysts (Fig. 204-7). These include low attenuation values characteristic of a cyst filled with water-like liquid, no enhancement with contrast material, and a thin to almost absent cystic capsule.
of Morgagni hernia (Fig. 204-6). Pineda and colleagues have emphasized the distinctive ability of current cross-sectional imaging techniques to delineate masses at the cardiophrenic angle83 and suggest that such masses should be interpreted as soft tissue components predictive of malignancy.83 Pugatch,87 Kaimal41 and, more recently, Kim and associates44 have described the essential CT features of pericardial cysts (Fig. 204-7). These include low attenuation values characteristic of a cyst filled with water-like liquid, no enhancement with contrast material, and a thin to almost absent cystic capsule.
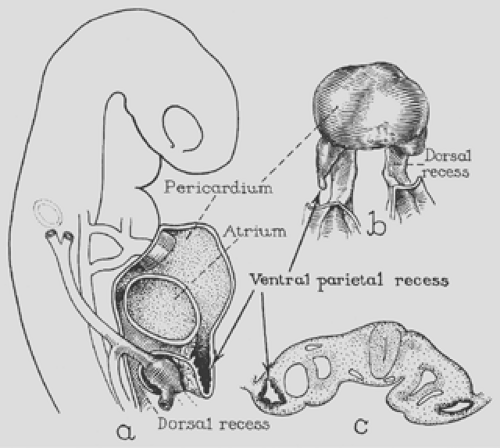 Figure 204-3. A: Parasagittal section of rabbit embryo, 9 days old. The ventral parietal recess pockets into the septum transversum are illustrated. B: The ventral surface of a cut of the pericardial coelom of a 20-somite human embryo illustrating the diverticulum-like appearance of the ventral parietal recesses. C: Transverse section of a 10-somite rabbit embryo, giving another representation of the spatial relationships of the parietal recess. (From Lillie WI, McDonald JR, Clagett OT. Pericardial celomic cysts and pericardial diverticula. A concept of etiology and report of cases. J Thorac Surg 1950;20:494. With permission.) |
Table 204-1 Lesions That May Result When the Parietal Recess Persists | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||
Given the correct indications,84 surgical resection is the preferred therapy (Fig. 204-8), either by an open procedure or by VATS. Very large cysts, as reported by Satur and associates,91 can readily be successfully resected by a VATS procedure. More recently, Bacchetta and colleagues have reported on the resection of a pericardial cyst by a robotic-assisted thoracic surgery.8 In addition, the experience with video-assisted mediastinoscopic removal of paratracheal mesothelial cysts has been described by several authors.39,67 With confirmation of the cystic nature of the lesion by CT scan and fine-needle aspiration (FNA) of clear watery fluid further confirming the diagnosis, Stoller and colleagues103 suggested that simple aspiration is an acceptable treatment because none of these cysts have any malignant potential. The aspiration of an unrecognized primary or secondary hy- datid cyst of the mediastinum in this area is highly unlikely except in individuals from or living in areas of high epidemicity of Echinococcus granulosus infestations. In such situations, specific serologic tests (see Chapter 94) for the disease may be conducted. Of course if doubts still persist, excision rather than aspiration should be performed.
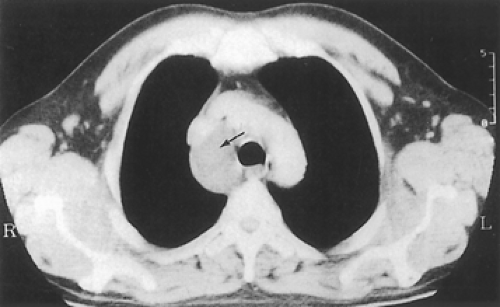 Figure 204-4. CT scan showing a pericardial cyst (arrow) in the right paratracheal area. (From Kutlay H, et al. Atypically located pericardial cysts. Ann Thorac Surg 2001;72:2137. With permission.) |
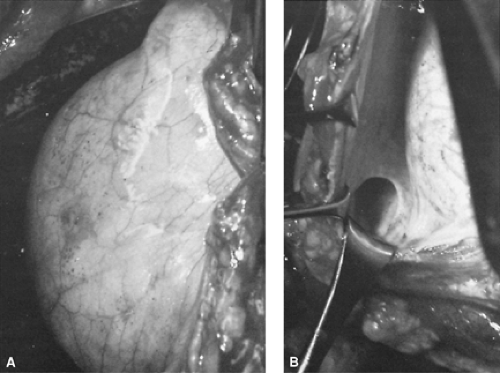 Figure 204-5. Pleuropericardial cyst with persistent communication to the pericardial sac, hence a true pericardial diverticulum. A: Diverticulum as seen at operation. B: Persistent communication between diverticulum and pericardial sac is well demonstrated. |
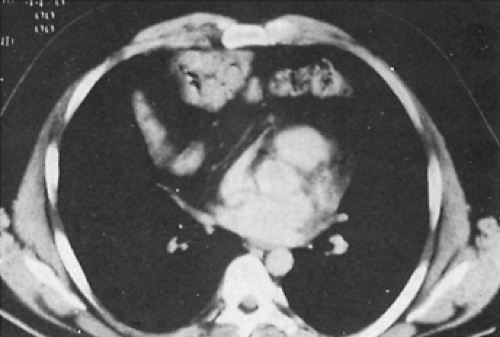 Figure 204-6. CT scan of the chest reveals the presence of a large bowel arising through a foramen of Margagni hernia. (Courtesy of D. Aberle, M.D., University of California, Los Angeles, UCLA School of Medicine.) |
Simple Mesothelial (Pleural) Cysts
Unilocular mesothelial cysts occurring primarily in the anterior compartment of the mediastinum have frequently been referred to as lymphangiomatous or unilocular cystic hygromas. These designations are most likely inappropriate because the histologic structures of the wall and the internal structure of the cyst fail to reveal the features of a true lymphangioma (isolated mediastinal cystic hygroma; see Chapter 176) and instead reveal only a single layer of flattened endothelial cells with an underlying connective tissue stroma without interlacing bands within the cystic structures.
These lesions are most often asymptomatic and discovered only on incidental radiography of the chest (Fig. 204-9). Jamplis and colleagues6 were the first to report a mesothelial cyst in the anterior compartment of the mediastinum as well as one in a costovertebral sulcus associated with vertebral body erosion. The concurrence of a cystic hygroma in the neck along with foregut and mesothelial cysts in a 14-year-old boy was noted by Awad and coworkers.6 In addition, migration of simple mesothelial pleural cysts due to a stalk from the pericardial fat pad has also been reported.109
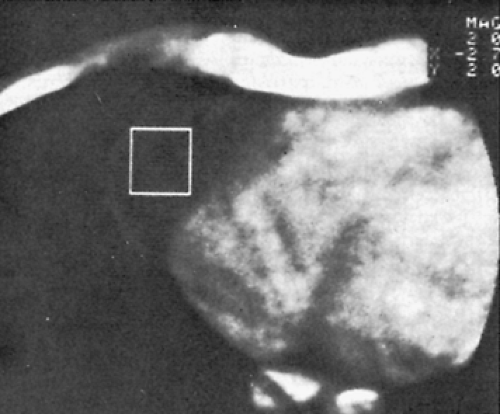 Figure 204-7. CT scan of the chest reveals a typical pleuropericardial cyst. The lesion is nonenhancing (white square), contiguous with the right side of the pericardium. The attenuation value is characteristic of a cystic lesion. (Adapted from Kaimal KP. Computed tomography in the diagnosis of pericardial cyst. Am Heart J 1982;103:565.) |
 Figure 204-8. Photograph of a surgically excised mesothelial (pleuropericardial) cyst of the mediastinum. |
Evaluation of these mesothelial cysts, after initial identification of a mediastinal mass by radiology, is by ultrasonography or CT examination. The cystic nature of the lesion is readily identified by either of these two studies.
When the lesion is small and asymptomatic, periodic observation is a reasonable course of action. Unilocular “typical” cysts may be also amenable to percutaneous drainage.109 When the lesion is large or thought to be the cause of symptoms, surgical excision is recommended via the most appropriate thoracic approach. Surgical excision is definitely diagnostic and curative.
Thymic Cysts
Thymic cysts of the mediastinum are uncommon. Bieger and McAdams10 reported that they constitute only 1% of mediastinal masses. Cohen and colleagues,17 however, reported an incidence of 4.8% in a series of 230 patients from Walter Reed Army Hospital, most of whom can be assumed to have been adults. Likewise, Hirano and associates35 reported an incidence of 4.9% in 242 mediastinal masses in a Japanese series. In Japanese children, the incidence of thymic cysts was less than 1% of 108 mediastinal masses as reported by Akashi and associates.2 In a surgical series of 105 mediastinal cysts, 28% were thymic in origin.103 Thymic cysts are inevitably found along the developmental tract of the thymus and hence can be located in the neck or in the anterior compartment of the mediastinum, as noted by le Roux and associates, Krech and Storey,48 and Bieger and McAdams.10 The cysts are most often mediastinal in location and, according to the review by Fahmy,21 more than half of the cervical thymic cysts extended into the mediastinum.93
Typically, the thymic cyst is unilocular and has a smooth fibrous capsule lined by epithelium that may be composed of cuboidal, columnar (with or without cilia), transitional, or squamous cells. Cholesterol clefts and granulomas with foreign body cells are commonly found within the cyst wall; these findings, according to Wick,111,112 are unusual in other cystic lesions in the
mediastinum. Thymic tissue within the wall is thought to be necessary to establish the diagnosis of a thymic cyst. The thymic tissue varies in amount but typically shows corticomedullary differentiation and Hassall’s corpuscles, both solid and cystic. Wick111,112 noted that Hassall’s corpuscles can be found in roughly 50% of the thymic cysts. Guba and colleagues31 described the finding of either thyroid or parathyroid tissue in many of the cervical thymic cysts.
mediastinum. Thymic tissue within the wall is thought to be necessary to establish the diagnosis of a thymic cyst. The thymic tissue varies in amount but typically shows corticomedullary differentiation and Hassall’s corpuscles, both solid and cystic. Wick111,112 noted that Hassall’s corpuscles can be found in roughly 50% of the thymic cysts. Guba and colleagues31 described the finding of either thyroid or parathyroid tissue in many of the cervical thymic cysts.
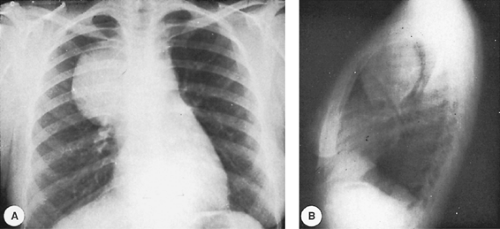 Figure 204-9. A,B: Posteroanterior and lateral radiographs of a young woman with a large unilocular mesothelial cyst of the mediastinum. The trachea is displaced posteriorly. |
Wick112 has described a subtype of the thymic cysts. This is the so-called proliferating variant. In these cysts there are narrow and often interconnecting tongues of squamous epithelium that project irregularly into the fibrous cyst wall, simulating an invasive carcinoma. However, the cells are cytologically bland and amitotic; the borders of the penetrating strands of squamous cells are essentially even, which would be uncharacteristic of a malignancy. All in all, this subtype (proliferating variant) behaves clinically like the more common nonproliferating cell types of thymic cysts. The fluid in the cysts is usually clear but may be turbid or sanguinous. In addition to the unilocular cysts, multilocular thymic cysts may also occur, but less commonly so. Suster and Rosai102 reported a series of 18 patients with multilocular thymic cysts. These appear as soft, rubbery masses in the anterior mediastinal compartment; on cut section, multiple cavities (multilocular) are filled with gray-brown or dark bloody fluid. The walls are thick and fibrous, and multiple septa and areas of solid tissue are present. The microscopic features, however, are not unlike those found in the unilocular cysts. Recently Kondo and associates46 reaffirmed the view that the acquired nature of these cysts appears to result from background thymic inflammations leading to obstruction and dilatation of the medullary duct,46 thus introducing the vexata quaestio of the origin of thymic cysts. Indeed, the cause of thymic cysts originally was somewhat controversial. Bieger and McAdams10 noted that Dubois, in the mid-nineteenth century,20 reported cystic lesions of the thymus (Dubois’s abscesses) in postmortem examinations of children who died secondary to congenital syphilis. At present, most believe that unilocular thymic cysts are either congenital or originate from cystic dilation of bronchial pouch remnants. The congenital theory is believed by most. On the other hand, the multiloculated cysts are acquired lesions. Infection, immune-mediated pathogenesis, trauma, and neoplasia have been noted to be the underlying associated causes of the multiloculated cysts by Suster and Rosai,102 Kornstein,47 Jaramillo and colleagues,40 and Kondo.46 The multilocular cyst is an acquired reactive process; often an inflammatory reaction is present, as are multiple adhesions to adjacent structures. The cysts arise in the thymic gland, in contrast to the extrathymic location of congenital unilocular cysts. Their association with neoplasia has been noted by Suster and Rosai,102 as especially seen in patients with nodular sclerosing Hodgkin’s disease and mediastinal seminomas. A few are seen in patients with acquired immunodeficiency syndrome (AIDS), as noted by Avila and coworkers5 (an incidence of 0.9%). Others are found to be associated with myasthenia gravis (four of eight patients described by Choi and associates15 presented with this association). A small number of cases have been associated with Sjögren’s syndrome, as noted in the patient reported by Kondo and colleagues46 and in two of the patients recorded by Suster and Rosai.102 Of particular interest is the occurrence of incidental thymic epithelial tumor (thymoma) and thymic carcinoma in the wall of the multiloculated thymic cyst.
The presence of thymoma is an unusual finding in a true unilocular (congenital) thymic cyst. This occurrence must be differentiated from a cystic thymoma. Eight cases have been described in the Japanese literature. The most recent three cases have been reported by Noriyuki,72 Kurihara,50 and Udaka107 and their associates. All of the latter three patients were young adults, and the thymoma made up only a small portion of the thymic cyst. Yamashita and colleagues113 and Babu and Nirmala7 have also described thymic carcinomas that arose in congenital thymic cysts. It would appear that the appropriate classification of such lesions as thymic cysts is to some extent suspect.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


