Mediastinoscopy and Other Thoracic Staging Procedures
Mediastinoscopy and Other Thoracic Staging Procedures
Michael Lanuti
INTRODUCTION
Lung cancer staging is continuously evolving as technological advances improve the imaging and endoscopic modalities available to better stratify patients into treatment and prognostic categories. The benefits of enhanced staging modalities, both local and metastatic, are to enrich the population of patients who can benefit from surgery and to avoid surgery in those patients who are not likely to benefit. The tumornode-metastasis (TNM) staging system for lung cancer has undergone multiple revisions since 1986 when it was first published by Clifton Mountain based on 2155 lung cancer patients derived from a single institution, University of Texas, MD Anderson Cancer Center. The current seventh edition staging system for lung cancer (revised in 2009, and summarized in Tables 2.1 and 2.2) has been validated in a data set of 81,015 lung cancer patients from 19 countries, but excludes some patient populations in Africa, South America, the Indian subcontinent, and parts of China. It is the basis on which treatment strategies are constructed and is highly dependent upon accurate staging.
Operative intervention is routinely offered for stage I (lymph node negative, T1a-bN0 and T2aN0) and stage II (T1a-bN1, T2aN1, T2bN0-1, T3N0) patients. Complete resection in stage I yields a cure rate of ˜58% to 73% and is not enhanced by adjuvant regimens except in a subset of stage IB tumors >4 cm. Recent evidence seems to support a survival advantage for adjuvant therapy in resected stage II and III disease. Node-negative superior sulcus tumors stage IIB (T3N0M0) tumors that can be resected en bloc are best treated surgically, with selective use of concurrent chemotherapy and external beam radiation given preoperatively. Stage IIIA disease (T1-2N2, T3N1-2, T4N0-1) is a heterogeneous group of locally advanced tumors where multimodality therapy including surgery should be carefully considered. At the other end of the spectrum, stage IIIB and IV patients, with rare exceptions, do not benefit from surgical resection. A subset of stage IV patients with oligometastatic disease of solid organs (such as brain and adrenal gland) and no N2 disease may benefit from resection of the metastatic site and lung to achieve a 5-year survival approaching 20%.
Techniques for the identification and subsequent staging of lung cancer have improved; however, no single modality has been able to noninvasively confirm definitively the presence of lymph node metastases. Computed tomography (CT), positron emission tomography (PET), and less frequently routine magnetic resonance imaging (MRI) of the chest have been employed as clinical staging modalities for lung cancer. Lung cancer staging should include a diagnostic quality CT, a PET to evaluate the mediastinal lymph nodes and exclude extrathoracic or bone metastases, and liberal use of more invasive types of mediastinal staging such as, mediastinoscopy, endobronchial ultrasound (EBUS), and/or esophageal ultrasound-guided fine needle aspiration (EUS-FNA) of lymph nodes, and in selected patients video-assisted thoracoscopy (VATS). All of these modalities have different sensitivity and specificity for lymph node staging. Lymph node metastasis portends a worse prognosis, and surgical resectability for cure is greatly influenced by mediastinal lymph node involvement.
Evaluation of mediastinal lymph node metastases by CT alone has been extensively reviewed in the literature and has historically yielded an overall sensitivity of 59% (range 20% to 81%) and an overall specificity of 78% (range 44% to 100%). PET evaluation of the mediastinum for stage I and II nonsmall cell lung cancer (NSCLC) has yielded a sensitivity of 85% and specificity of 88%. Its negative predictive value for the mediastinum is 87%, whereas the positive predictive value is 56%. Specificity of PET is limited as both neoplastic and inflammatory nodes can have increased fluorine-18-labeled deoxyglucose (FDG) uptake. Meta-analysis of 44 relevant studies that explored the diagnostic accuracy of PET compared with CT imaging in detecting mediastinal lymph node metastases demonstrated that PET was more accurate. Accurate detection of hilar nodal involvement in lung cancer has historically been difficult, but with CT-PET and more widespread use of EBUS transbronchial needle aspiration biopsy, pathologic correlation has proven that PET is very good at detecting N1 disease.
The widespread use and availability of PET-CT fusion imaging has increased the proportion of patients found to have additional lesions that contraindicate surgical treatment but require tissue confirmation to exclude a false-positive examination. For optimal results from PET-CT, patients fast for 4 to 6 hours and then receive 15 mcuries of 18-FDG (550 MBq) as an intravenous injection 1 hour before study. 18-FDG has a 110-minute half-life. Transmission CT (5 mm cuts) is acquired during quiet breathing and then the PET evaluation is acquired. CT-PET acquisition takes about 30 to 35 minutes. Importantly, the transmission CT scan that is generated by this modality is not as accurate as a diagnostic quality CT chest. This technology has been evaluated in the literature with increasing frequency. In a sentinel study from Switzerland in 2003, the authors studied PET-CT in 50 patients with NSCLC. Integrated PET-CT provided additional information in 41% of patients and was significantly more accurate in precise staging compared with CT alone, PET alone, or visual correlation of PET and CT.
MRI of the lung has historically been challenged by poor spatial resolution and high noise-to-contrast ratio and has been reserved for characterizing mediastinal masses or detecting tumor invasion into chest wall, mediastinum, vasculature structures, diaphragm, pericardium, or bone. MRI has greatly contributed to the clinical staging of superior sulcus tumors. A recent report suggests that new MRI techniques such as diffusion-weighted imaging (DWI) and short tau inversion recovery turbo spin echo (STIR) sequences can improve upon the accuracy of PET/CT for distinguishing benign from malignant lymph nodes. Furthermore, PET-MRI is the newest modality that is being evaluated for lung cancer staging.
Table 2.1 TNM 7th Edition International Lung Cancer Staging System
Tis
Carcinoma in situ
T1
Tumor <3 cm surrounded by lung, no bronchoscopic invasion
T1a
Tumor <2 cm
T1b
Tumor >2 cm but <3 cm
T2
Tumor >3 cm but <7 cm, or tumor with any of the following features: involves main bronchus <2 cm from carina
Invades visceral pleura, or associated with obstructive pneumonitis extending to hilum
T2a
Tumor >3 cm but <5 cm
T2b
Tumor >5 cm but <7 cm
T3
Tumor >7 cm or one that directly invades any of the following: chest wall (including superior sulcus), diaphragm, phrenic nerve, mediastinal pleura, parietal pericardium or tumour <2 cm from carina without involvement of carina, or Separate tumor nodules in same lobe
T4
Tumor of any size that invades any of the following: mediastinum, heart, great vessels, trachea, RLN, esophagus, vertebral body, carina or Separate tumor nodules in different ipsilateral lobe
N1
Mets to ipsilateral peribronchial or hilar LNs and intrapulmonary LNs, including involvement by direct extension
N2
Mets to ipsilateral paratracheal or subcarinal LNs
N3
Mets to contralateral paratracheal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular LNs
M1a
Separate tumor nodules in a contralateral lobe, tumor with pleural nodules, or malignant pleural or pericardial effusion
M1b
Distant metastases
LNs, lymph nodes; RLN, recurrent laryngeal nerve.
(American Joint Committee on Cancer, 7th Edition Lung Cancer Staging Manual, 2010, Chicago, IL.)
Table 2.2 7th Edition International Lung Cancer Staging System with 5-Year Survival Based on Pathologic Staging
Stage
T
N
M
5-y survival
0
Tis
N0
M0
IA
T1a,b
N0
M0
73%
IB
T2a
N0
M0
58%
IIA
T1a,b
N1
M0
46%
T2a
N1
M0
T2b
N0
M0
IIB
T2b
N1
M0
36%
T3
N0
M0
IIIA
T1,T2
N2
M0
24%
T3
N1,N2
M0
T4
N0,N1
M0
IIIB
T4
N2
M0
9%
Any T
N3
M0
IV
Any T
Any N
M1a,b
MEDIASTINOSCOPY
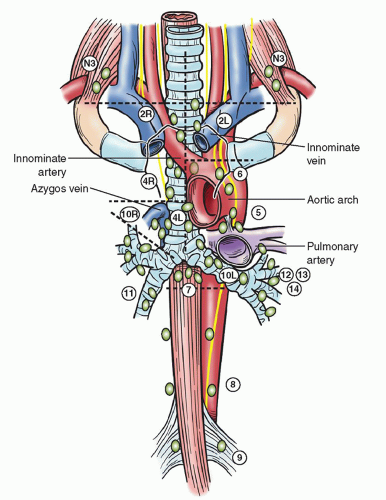
The gold standard for staging the mediastinum is cervical mediastinoscopy, which was developed by Harken and associates in 1954 and then promulgated by Carlens in 1959 and later Pearson in 1965. Carlens and Pearson recognized that mediastinoscopy potentially was useful not only for lung cancer staging but also for the diagnosis of lymphoma, metastatic disease from an extrathoracic origin, infectious etiologies, and sarcoidosis. It is the benchmark against which all comparisons of lymph node accuracy are currently analyzed. The mediastinoscopes used today are modifications of the original instruments, with distal illumination, a beveled end, and a lateral slit for instrumentation (see Fig. 2.1). The efficacy of mediastinoscopy has been well established in the assessment of enlarged mediastinal lymph nodes with 100% specificity and ~90% sensitivity. In patients with known or suspected lung cancer, the routine use of mediastinoscopy can change the plan of care in up to 25% of patients. Large studies confirm false-negative rates from 5% to 8%, as demonstrated in Table 2.3. The false-negative rate of mediastinoscopy may be attributed to the diligence of the surgeon dissecting and sampling the nodes. Ideally, five nodal stations (stations 2R, 4R, 7, 2L, and 4L) should be routinely examined (see Fig. 2.2), with at least one node sampled from each station unless none are present after dissection in the region of a particular nodal station. Compared with conventional mediastinoscopy, video mediastinoscopy appears to yield some improvement in sensitivity (92%) and false-negative rates (7%).
Routine mediastinoscopy remains somewhat controversial in that many lung cancer treatment centers use the modality selectively. A national survey of 729 hospitals (31% teaching or university hospitals, 38% community cancer centers, 46% comprehensive community cancer centers) sponsored by the American College of Surgeons identified more than 11,668 patients whose initial management included surgical therapy for lung cancer. The mediastinum was evaluated preoperatively with mediastinoscopy in only 27% of these surgical patients and only 26% underwent a staging PET. The underuse of aggressive mediastinal staging in both academic and community lung cancer care is sobering. Additionally troublesome is that only 42% had lymph nodes sampled at any mediastinal level during the definitive surgical procedure.
Fig. 2.2. The Mountain-Dresler modification of the regional lymph node map originally proposed by the American Thoracic Society. (Redrawn after Mountain CF, Dresler CM. Regional lymph node classification for lung cancer staging. Chest 1997;111:1718-1723c.)
Indications and Contraindications
Mediastinoscopy should be performed in any patient harboring a suspicious lung nodule with enlarged (>1 cm in short axis measured on CT) or FDG-avid mediastinal lymph nodes (N2 or N3), those with central tumors, and those with peripheral tumors >2 cm. T1 tumors with an aggressive histology (i.e., large cell neuroendocrine carcinosarcoma, small cell or pleomorphic carcinomas) should also undergo mediastinoscopy. Peripheral T1a lesions (tumors ≤2 cm) with PET-negative mediastinal lymph nodes can be regarded as the one exception to the routine use of mediastinoscopy. Mediastinoscopy is the procedure of choice for lung cancer staging (endorsed by the American College of Chest Physicians, and European Society of Thoracic Surgeons) but endoscopic techniques such as EBUS or EUS-FNA are recognized as modalities where a cytologic diagnosis can be achieved to initiate a treatment strategy. If EBUS or EUS-directed biopsies are negative in a pathologically enlarged or FDG-avid mediastinal lymph node, mediastinoscopy is still recommended.
Mediastinoscopy does not have many strict contraindications except for perhaps inability to extend the neck because of severe kyphosis or fused cervical vertebra. Relative contraindications to mediastinoscopy include large thyroid goiter, severe atherosclerotic disease in the aortic arch, vertebral arteries (vulnerability to ischemic events with neck extension), or the innominate artery which can contribute to embolic stroke. End tracheal stoma after laryngectomy in association with neck radiation can present anatomic difficulty with increased risk of cervical wound infection. Previous mediastinoscopy is associated with fibrosis of the pretracheal tissue plane and makes redo mediastinoscopy challenging. Despite this phenomenon, repeat mediastinoscopy is feasible and safe in most cases and can be carefully used to restage the mediastinum after induction therapy. Particular care must be exercised in separating the innominate artery from the trachea. Sharp dissection under direct vision is safer than the blunt approach used in first-time mediastinoscopy. Many surgeons reserve EBUS-directed biopsy for preinduction mediastinal lymph node sampling in patients suspected of harboring locally advanced lung cancer (stage IIIA) with positive N2 nodes.
Technique
Mediastinoscopy is an outpatient procedure that needs to be performed in a hospital setting to efficiently manage the potential for hemorrhage. The patient is placed supine on the operating room table where the head is placed at the top of the bed (Fig. 2.3). After establishing general endotracheal anesthesia, the neck is extended with either a thyroid bag or a roll under the shoulders. A pulse oximeter or radial artery cannula can be used to monitor compression of the innominate artery (observation of a dampened wave form) so as not to compromise blood flow to the right carotid artery for an extended period. Most surgeons include the entire sternum in the operative field in the event that serious hemorrhage is encountered and median sternotomy is necessary. In the event that a patient already has a previous median sternotomy, a right or left anterior thoracotomy can be considered for exploration in the setting of acute hemorrhage. Mediastinoscopy can be achieved with direct visualization through a standard scope (Fig. 2.1
Only gold members can continue reading. Log In or Register to continue