Management of Coronary Artery Disease: Medical Therapy, Percutaneous Coronary Intervention, and Coronary Artery Bypass Grafting
Management of Coronary Artery Disease: Medical Therapy, Percutaneous Coronary Intervention, and Coronary Artery Bypass Grafting
S. Hinan Ahmed FSCAI, FACC
Steven R. Bailey MD, FACAI, FACC, FACP
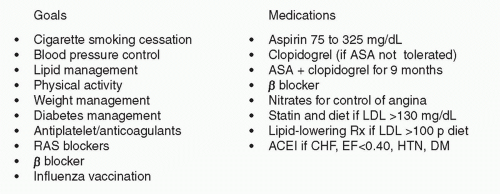
The presence of coronary artery disease (CAD) carries an increased risk of subsequent clinical events including myocardial, cerebrovascular and peripheral ischemia or infarction (1). The diagnosis of CAD is most often established with patients who present with signs or symptoms of coronary artery narrowing, which include symptoms of myocardial ischemia (exertional chest pressure or tightness, shortness of breath, diaphoresis) relieved with rest or medications, prior myocardial injury, including non-ST-segment elevation myocardial infarction (NSTEMI), or ST segment elevation myocardial infarction (STEMI), or evidence of myocardial ischemia using noninvasive or invasive imaging. The presence of atherosclerotic vascular disease in other arterial beds (Carotid, Central Aorta, or Peripheral Vascular) identifies a population at increased risk of associated CAD who therefore should also be considered at increased risk for coronary events and treated medically as if they have established CAD. Multi-Society Guidelines have been published addressing secondary and post-revascularization guidelines for medical care for these patients (2). The current components of guideline-based care are presented in Figure 30-1.
The therapeutic options for treating myocardial ischemia are directed toward improving the patients’ symptoms and quality of life, sustaining or improving ventricular function, and decreasing the risk of subsequent cardiovascular events whenever possible. In chronic stable angina, the use of medical therapy is primarily focused upon improving patients’ symptoms and quality of life. When medical therapy is insufficient to limit the ischemic symptoms/provide an adequate quality of life or if the patient is found to have high-risk features, myocardial revascularization with percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) may be required. In patients who present with acute myocardial ischemia or injury in the setting of acute coronary ischemia (ACS) or STEMI, revascularization has been demonstrated to improve outcomes for the populations that have been studied.
FIGURE 30-1 Components of guideline based care from the ACC/AHA/SCAI Guidelines 2011.
Contemporary clinical approach’s for decision making regarding the specific treatment regimen for an individual patient is influenced by multiple factors, including the clinical presentation, the patient’s comorbidities, as well as the underlying coronary anatomy, ventricular function, and systemic manifestations of atherosclerosis such as carotid and peripheral vascular disease.
Many of the randomized trials comparing medical therapy with revascularization or between revascularization strategies occurred prior to our current understanding of the pathology of acute coronary events and often did not include current medical regimens for treatment of chronic stable angina. Additionally, risk stratification in chronic stable angina based upon the extent of myocardial ischemia had not been included into our investigations, nor were the imaging tools available to incorporate this tool into prior clinical investigations.
MEDICAL THERAPY OF CAD
Medical therapy, as the term is currently used, is a bit of a misnomer as applied to treatment of CAD, as best practices for care involve lifestyle changes combined with the use of medications to decrease the risk of subsequent cardiac and vascular events. The medications associated with improved outcomes in clinical trials include aspirin, statin, thienopyridines, β blockers, and angiotensin- converting enzyme inhibitors (ACE-I) or angiotensin receptor blockers (ARB). This approach to improved clinical outcomes has also been referred to as “optimal medical therapy” or “guideline-determined medical therapy” or GDMT. These therapies are also addressed in therapies for secondary prevention therapies of atherosclerosis.
While adherence to these therapies is recognized as decreasing the risk of subsequent cardiovascular events, investigations of adherence to these recommendations indicate very poor compliance. The current components of the preventative cardiovascular health metric are smoking status, physical activity, body mass index (BMI), healthy diet, total serum cholesterol, blood pressure, and fasting blood glucose level. The recent report by Yang et al. (3) examining a national representative sample of 44,959 US adults concluded that only 1.2% of the population met all seven current cardiovascular health metrics with a corresponding worse outcome than those who met more than six of the metrics. As discussed below, there are similar issues with compliance even in those patients who are known to have cardiovascular disease. The recommended components of guideline-based medical care based upon the current guidelines are listed in Table 30-1.
TABLE 30-1 Randomized Trials of Medical Therapy versus CABG
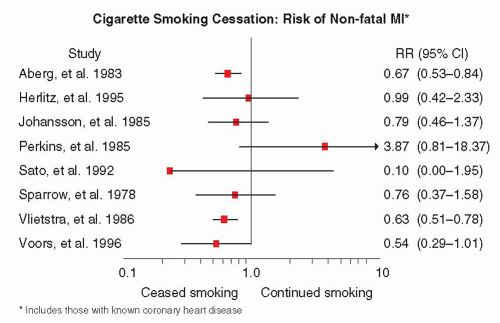
Continued smoking constitutes the most significant risk for the development of future events. The estimated risk of cardiovascular events because of smoking varies from 1.5- to 3.0-fold (4). Recently a meta-analysis by Huxley (5) demonstrated that there was an additional 25% risk in women than in men and that this risk increased 2% per year of smoking. Smoking cessation does confer a risk reduction in mortality of 36% (6), and those who quit smoking under age 50 had a 50% lower risk of dying than those who continued. A meta-analysis from Critchley et al. (7) also demonstrated a consistent benefit of smoking cessation in decreasing subsequent nonfatal myocardial infarction (Fig. 30-2).
FIGURE 30-2 Impact of smoking cessation on the risk of nonfatal myocardial infarction. (Modified from: Critchley, et al. JAMA. 2003;290:86-97, with permission.)
WEIGHT REDUCTION
Obesity is associated with many conditions that increase the risk of cardiovascular events and mortality. The increased incidence of type 2 diabetes, hypertension, left-ventricular hypertrophy, and sleep apnea all contribute to atherosclerosis and sudden cardiac death. Obesity alone has been demonstrated to impair endothelial dysfunction (8).
HYPERTENSION
Elevated blood pressure is the most common primary diagnosis in the United States according to the national ambulatory medical survey (9), and it remains one of the most important factors driving subsequent cardiovascular events in patients with atherosclerosis. It is a continuous risk factor that is independent of other risks and increases with age. The cardiovascular impact on the heart includes not only angina and myocardial infarction (MI) but also ventricular hypertrophy, and diastolic and systolic heart failure, which compounds any coronary artery narrowing. The presence of hypertensive kidney disease also impacts our care of patients who will undergo or who have undergone coronary artery revascularization. Antihypertensive therapy is associated with up to a 25% reduction in MI. If CVD is present only nine patients need to be treated to avoid one death with adequate therapy.
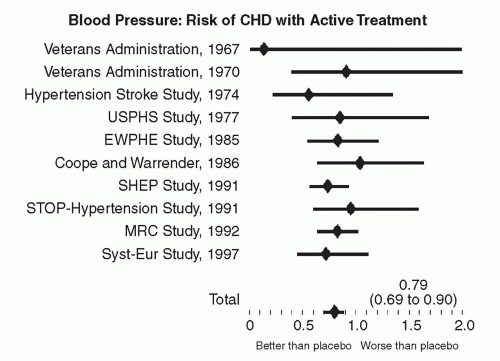
The current definitions of blood pressure include normal (systolic <120 and diastolic <80 mm Hg) prehypertension (systolic >120-139 or diastolic 80-89 mm Hg) and hypertension (systolic ≥140 or diastolic ≥90 mm Hg). The current goal for blood pressure is <140/90 (<130/80 for diabetes or chronic kidney disease). For patients with ischemic heart disease, LV dysfunction or those who are postmyocardial infarction, the current recommendations are for the use of ACE-I, ARB, and β blockers according to the ALLHAT (10), HOPE (11), ANBP2 (12), LIFE (13), and CONVINCE (14) trials. Figure 30-3 demonstrates the impact of treatment of hypertension in decreasing the risk of subsequent cardiovascular events.
HYPERLIPIDEMIA
Therapy to treat hypercholesterolemia, particularly elevated low-density lipoprotein (LDL), has been evaluated as primary and secondary therapy to prevent cardiovascular events. The relationship of LDL cholesterol to coronary events is presented in Figure 30-3. The National Cholesterol Education Program (NCEP) Adult Treatment Panel III has identified LDL cholesterol as the major cause of coronary heart disease (CHD) (15). LDL cholesterol lowering therefore is the primary target of lipid-lowering therapy. The current NCEP goals are a target LDL of <70 mg/dL for very high-risk patients, who are defined as those with known CAD and multiple major risk factors, severe or poorly controlled risk factors, multiple risk factors for metabolic syndrome, or acute coronary syndromes. The threshold for treatment of these patients should be an LDL cholesterol of ≥ 100 mg/dL.
Several large randomized trials have demonstrated that reduction of the LDL component is proportional to the decrease in subsequent cardiovascular events. Simvastatin was evaluated in the randomized Scandinavian Simvastatin Survival Trial ??????(4S) of 4,444 patients with a primary endpoint of all-cause mortality at a follow-up longer than 5 years. In this trial, simvastatin reduced the total cholesterol by 25% and the LDL by 35%, with an increase in the high-density lipoprotein (HDL) of 8%. There was a reduction in mortality from 8.2% to 11.5% (relative risk reduction of 30% (p = 0.0003) with fewer coronary deaths, nonfatal MIs, and need for revascularization (16). A number of other trials have shown the same benefit of cholesterol lowering for secondary prevention. The Cholesterol and Recurrent Events (CARE) Study randomized 4,159 patients with a recent (>3 month) MI and a baseline total cholesterol of <240 mg/dL and an elevated LDL (115-147) to placebo or pravastatin 40 mg/day. The primary endpoint of this trial was coronary death and nonfatal MI. The investigators found a 25% reduction in MI, a 31% reduction in stroke, and a 27% reduction in revascularization with a 20% reduction in coronary death (p = 0.10) that did not meet the prespecified endpoint.
FIGURE 30-3 Effect of treatment of blood pressure on risk of CHD. (Modified from: He J, et al. Am Heart J. 1999;138:211-219, with permission.)
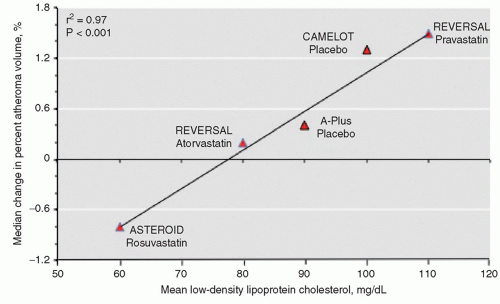
Plaque modification and its relation to clinical events have been evaluated using aggressive lipid-lowering therapy, the largest trials have been the REVERSAL (17) and the ASTEROID trials (18). The REVERSAL trial evaluated 502 patients randomized to either pravastatin, 40 mg, or atorvastatin, 80 mg, for 18 months with a primary endpoint of intravascular ultrasound (IVUS)-determined %plaque change using matched IVUS images. Lower LDL and C-reactive protein (CRP) levels were seen in each group, with the greatest change in the atorvastatin arm. Small (0.4% vs. 2.7%) changes were seen between the pravastatin group and the atorvastatin group (p = 0.02). The ASTEROID trial enrolled a similar number of patients (N = 507) all receiving rosuvastatin 40 mg/day with paired IVUS evaluations at baseline and 24 months after enrollment in 349 patients. The patients’ LDL-C levels decreased to a mean of 60.8 mg/dL along with a significant increase in HDL-C levels of 14.7%. These changes corresponded to a decrease in Plaque Atheroma Volume (PAV) of 3.15% and were significant in all subgroups that achieved an average LDL level of <70 mg/dL during the study. The study was not powered to examine clinical outcomes. The impact of aggressive lipid-lowering therapy for plaque is illustrated in Figure 30-4.
The clinical effect of aggressive LDL lowering was investigated in several settings. The MIRACL trial (19) was a short-term investigation (16 weeks) in which 3,086 patients with unstable angina or non-q-wave MI were randomized to atorvastatin 80 mg/day or placebo. The primary endpoint of this trial was death, nonfatal MI, or stroke.
The Treating to New Targets (TNT) trial (20) examined the late efficacy and safety of high-dose atorvastatin therapy in over 10,000 patients, with a primary endpoint of major cardiac endpoints (MACE). This trial assigned patients to a dose of either 10 mg/day or 80 mg/day, with a follow-up of 4.9 years, and demonstrated that in the high-dose arm, in those who achieved a mean LDL of 77 mg/dL, the MACE rate was reduced by 22% (p <0.001).
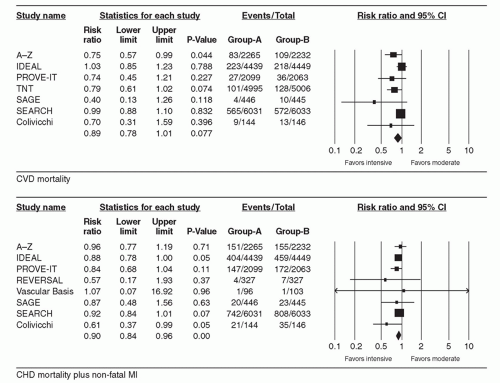
A recent meta-analysis by Chan et al. compared over 50,000 patients who received intensive lipid lowering therapy with those who received moderate therapy (21). A second larger metaanalysis of over 170,000 patients was performed by the Cholesterol Treatment Trialists’ (CTT) Collaboration (22). This study concluded that intensive therapy with statins resulted in reductions in nonfatal events, the composite of CHD death plus nonfatal MI, and the composite of fatal and nonfatal strokes. The outcomes are illustrated in Figure 30-5A and B, which demonstrates the outcomes for cardiovascular death with and without associated nonfatal MI. On a cautionary note, these benefits did not appear to result in significantly reduced mortality for secondary prevention populations.
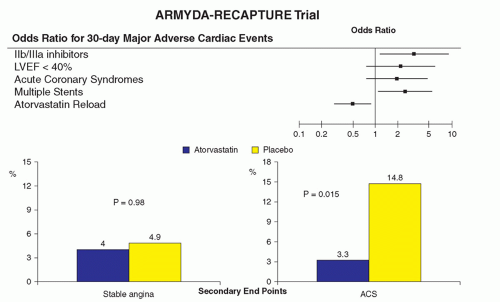
There are data that demonstrate the benefit at 30 days for the administration of 80 mg atorvastatin when “reloaded” prior to PCI from the ARMYD-Recapture trial. This benefit was seen in patients with stable angina and acute coronary syndromes. There was no benefit seen with the use of IIb/IIIa inhibitors. Patti et al. (23) reported a meta-analysis of over 3,341 patients from 13 published trials. This study demonstrated a significant reduction of major adverse cardiac events from 12.6% to 7.4% (p <0.00001) as shown in Figure 30-6. This investigation also examined for the presence of publication bias, which was not seen.
FIGURE 30-4 Impact of lipid lowering therapy on plaque regression. (Adapted from: Nissen SE, et al. JAMA. 295;1556- 1565, with permission.)
FIGURE 30-5 A: Impact of intensive lipid lowering therapy on CVD sortality. B: Impact of intensive lipid lowering therapy on CVD mortality and nonfatal MI. (From: Mills EJ, et al. Eur Heart J. 2011;32:1409-1415, with permission.)
ANTIPLATELET THERAPY
Antiplatelet therapy is accepted as an effective therapy in patients with known CAD. A collaborative meta-analysis of antiplatelet therapy included 287 published trials that involved more than 130,000 patients (24). This analysis demonstrated a 22% reduction in the composite of nonfatal MI, stroke, or vascular death. Aspirin was the most frequently studied therapy in doses of 75 to 150 mg per day. The current ACC/AHA/SCAI guidelines contain a Class IA recommendation for aspirin in doses of 75 to 325 mg daily.
FIGURE 30-6 Benefit of lipid re-administration prior to PCI. (Modified from: Di Sciascio G, et al. J Am Coll Cardiol. 2009;54:558-565, with permission.)
Secondary prevention is recommended, in patients with known CAD, using clopidogrel, 75 mg daily, or Ticlopidine, 250 mg twice daily. In patients that are aspirin intolerant or have a true aspirin allergy following a NSTEMI (Class 1A) or STEMI (Class I Level C), single agent therapy with clopidogrel, 75 mg daily, or Ticlopidine, 250 mg twice daily is also indicated. In patients with known CVD without MI or multiple risk factors, the data regarding antiplatelet therapy are less compelling. The CHARISMA trial (25), which compared aspirin alone with aspirin plus clopidogrel, did not demonstrate a benefit with combined therapy.
BETA BLOCKER THERAPY
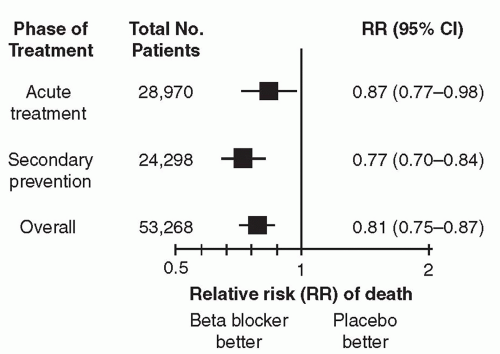
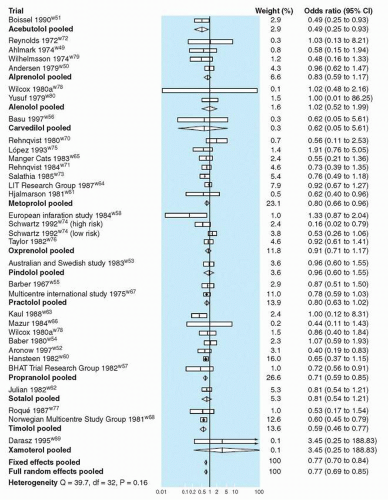
Studies evaluating the use of β blocker therapy have consistently indicated that it improves outcomes in three important patient populations: (a) those after acute myocardial infarction, (b) those in the setting of LV systolic dysfunction, and (c) those undergoing therapies for secondary prevention of cardiovascular events. Figure 30-7 demonstrates the benefit of β blockers overall as well as individually in acute therapy as well as for secondary prevention. The results of a meta-analysis of over 53,000 patients demonstrating improvement in outcomes in secondary prevention and after acute coronary events are presented in Figure 30-8. The number needed to treat is 42 patients. Notably, only four drugs (propranolol, metoprolol, acebutolol, and timolol) demonstrated a benefit. The duration of therapy remains controversial in patients with stable angina in the absence of MI or left-ventricular dysfunction. High-risk patients, especially those with depressed LV function, do benefit from medical therapy for 3 years as established by the BHAT trial. One of the few long-term studies was published by Gottlieb et al. (26), which evaluated over 201,752 patients followed up for 2 years after initiation of therapy. While only 34% of patients received therapy, outcomes were better in all patients irrespective of indications, risk groups, or relative contraindications to β blocker therapy. The current consensus opinion is that β blocker therapy, in the absence of a contraindication, may provide sustained improvements in cardiovascular outcomes, partially related to neurohumoral blockade.
MEDICAL THERAPY VERSUS CABG
Even in trials of aggressive medical therapy using the appropriate medications and lifestyle modifications, many patients with chronic stable angina will develop symptoms that are not responsive to their medical regimen or will present with acute myocardial ischemic events. The randomized trials that compare medical therapy with CABG are primarily from the 1970s and 1980s, when the medications available to treat patients were restricted compared with those available over the last decade—as statins, thienopyridines, and ACE-1/ARB were not available, and even ASA and β blockers were not routinely administered. A comparison of the randomized trials of medical therapy versus CABG is seen in Table 30-2. These trials included four patients with chronic stable angina (27, 28, 29 and 30) and two with unstable angina (31, 32). As seen from this table, most study patients with depressed left-ventricular function and left main disease were excluded from these trials. Patients with left main disease were often excluded because of concerns regarding randomizing high-risk patients. These trials did demonstrate improvement in clinical symptoms compared with medical therapy alone, but did not establish that CABG was likely superior to medical therapy for improving mortality in this patient population except the recently published STICH trial (30), which demonstrated no difference in overall death, but did show improved outcomes for cardiovascular death and hospitalization in the CABG group.
FIGURE 30-7 Summary of trials of β blocker therapy. (From: Antman, et al. Acute myocardial infarction. In: Braunwald E, et al. ed. Heart Disease: A Textbook of Cardiovascular Medicine, 6th ed., Philadelphia, PA: W.B. Sanders; 2001: 1168, with permission.)
FIGURE 30-8 Effect of β blocker therapy on mortality after myocardial infarction. (From: Freemantle N, et al. BMJ. 1999;318(7200):1730-1726, with permission.)
Clinical decisions may also be based upon nonrandomized data such as those derived from registries. The most cited data are from the New York State registry (33) and the Duke Data Base (34). These registries examined outcomes in patients after referral for procedures. Such registries suffer from inherent bias with respect to patient referral and selection, inability to control for comorbidities and potential confounding variables that were not prospectively addressed such as age, frailty, renal function, and hemoglobin that were identified for randomized studies as being clinically important.
The general consensus gleaned from both randomized and registry data is that CABG offers advantages with respect to prolonged survival in patients with left main stenosis >50%, three-vessel CAD, and two-vessel CAD if the proximal left anterior descending artery has significant stenosis. These patient populations have not been subjected to any randomized study comparing medical therapy with CABG, so this still represents the best clinical assessment of available data.
A recent randomized trial, the STICH trial, did compare the outcomes of patients with depressed left-ventricular function who were randomized to contemporary medical therapy versus a group with contemporary medical therapy and CABG (30). While this study did not demonstrate any significant difference in mortality between medical therapy alone and medical therapy plus CABG, death due to cardiovascular causes and hospitalization for cardiac causes were lower among patients assigned to CABG than among those assigned to medical therapy (Fig. 30-9). It should be noted that 17% of the patients randomized to the medical therapy arm did undergo CABG during the follow-up period. While the analysis is appropriate as an intention to treat model, this may have impeded the ability to discern a statistical difference in such a small study population. Crossover during long-term follow-up therapy is a significant confounding variable in many of the trials evaluating medical therapy and revascularization.
TABLE 30-2 Randomized Trials of Medical Therapy versus Percutaneous Coronary Intervention
Trial
n
Major Outcome
Result
Comments
ACME USA 1987-1990
212
Exercise tolerance
PCI better
Prestent
ACME USA 1987-1990
101
Exercise tolerance
No difference
Prestent
RITA-2 UK, Ireland 1992-1996
1018
Death or MI
PCI better PCI had less angina
9% with BMS stents
AVERT USA, Europe 1995-1996
341
Any ischemic event
No difference
39% of PCI with BMS stents 25% of PCI with no lipid lowering
ACIP USA, Canada, UK 1991-1993
558
2-year mortality
No difference
Revascularization by CABG or PCI Revascularization gave better event-free survival Angina-guided; ischemia-guided revascularization
MASS Brazil 1988-1991
214
Event-free survival
CABG better
Revascularization by CABG or PCI Patients with LAD only
COURAGE trial
2287
Death any cause and nonfatal myocardial infarction
No difference
Less angina with revascularization 30% cross over from med to revascularization Largest ischemic burden benefited from revascularization
MEDICAL THERAPY COMPARED WITH PERCUTANEOUS INTERVENTIONS IN CHRONIC STABLE ANGINA
The introduction of percutaneous interventions resulted in rapid adoption of this revascularization strategy for large numbers of patients with angina previously treated exclusively with medications for angina. These studies may have used aspirin and β blockers, but other therapies were not standardly prescribed in these patients. Despite the widespread adoption of PCI, the number of trials performed to compare outcomes in chronic stable angina has been limited (Table 30-2). The most recent of these was a larger COURAGE trial (35), which investigated patients randomized to aggressive, contemporary medical therapy compared with PCI or CABG in a population of patients who had all undergone baseline coronary angiography. The trials of PCI versus medical therapy have been limited in the number of patients enrolled as well as the clinical complexity. Most studies investigated patients with normal ventricular function and single vessel CAD, with systematic inclusion of high-risk patients. The trials are further limited as they often used short-term endpoints designed to encompass only the early likelihood of having a clinical event. Owing to the constraints of these trial designs, it is not surprising that there are no data that unanimously support an improved survival benefit or decreased risk of future MIs in patients undergoing PCI compared with medical therapy. The trials of PCI versus medical therapy did demonstrate that percutaneous revascularization does improve functional capacity and decrease anginal frequency compared with medical therapy alone because of the frequency of small periprocedural elevations of myocardial enzymes. The COURAGE trial (35) excluded higher-risk patients because of clinical and angiographic screening, but did randomize 2,287 patients to “optimal medical therapy” (OMT) compared with “optimal medical therapy plus revascular-ization” over an approximate 5-year follow-up period. There was no difference in the primary endpoint of mortality, but patients had less frequent angina in the revascularization arm despite the fact that 32% of the OMT group required revascularization (PCI or CABG) during the follow-up period. Partly owing to the frequent revascularization in the OMT arm, there was no difference in angina status at five years despite a difference at all the earlier time points. This lack of effect at the late time point may have been influenced by the high revascularization rate in the control arm.
Only gold members can continue reading. Log In or Register to continue
May 28, 2016 | Posted by drzezo in CARDIOLOGY | Comments Off on Management of Coronary Artery Disease: Medical Therapy, Percutaneous Coronary Intervention, and Coronary Artery Bypass Grafting