Low-Dose Computed Tomography Screening: Experiences from the Randomized Population-Based Nelson Screening Trial
Low-Dose Computed Tomography Screening: Experiences from the Randomized Population-Based Nelson Screening Trial
Rob J. van Klaveren
Harry J. de Koning
NELSON TRIAL DESIGN
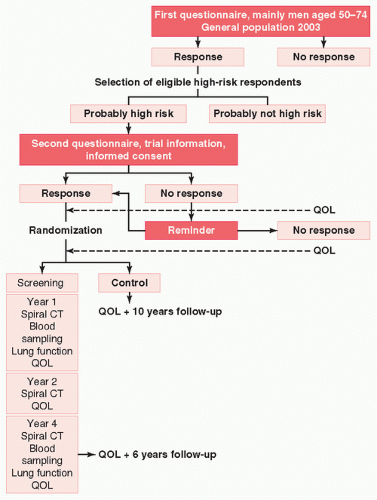
The Dutch-Belgian lung cancer screening trial (NELSON) investigates whether 16-detector, low-dose, multislice computed tomography (MSCT) screening in year 1, 2, and 4 will decrease lung cancer mortality compared to a control group without screening. Secondary end points of the study are to estimate the cost-effectiveness of this screening program and to assess the impact on quality of life. The design of the NELSON trial is shown in Figure 17.1. NELSON is the only large-scale, randomized, controlled, population-based lung cancer CT-screening trial in Europe, with 15,523 participants. Recruitment started in the second half of 2003, and the first CT screenings were made in April 2004. As of October 2007, the baseline-screening round has been completed, the second round is near its completion, and the third round has recently been started. The screening part of the trial will be finished by the end of 2009, but the follow-up period will continue until the end of 2015. During the first round, lung function tests have been performed, and biosamples (blood, plasma, serum, and sputum cytology) have been taken. The blood sampling and lung function test are repeated during the last screening round.
Recruitment During the first recruitment phase (second half of 2003), addresses of all men born between January 1, 1928 and January 1, 1953 were obtained from the population registries in seven districts in the Netherlands (Groningen, Drenthe, Utrecht, Eemland, Midden-Nederland, Kennemerland, and Amstelland-de Meerlanden) (Fig. 17.1). In addition, addresses of all men and women of the same age were obtained from the population registries of 14 municipalities around Leuven in Belgium. They received a first questionnaire about general health, alcohol consumption, physical exercise, cancer history, family history of lung cancer, body weight and length, education, and their opinion on screening programs in general. The questionnaire contained 11 questions on smoking from the Minimum Common Dataset (May 2002) of the EU-U.S. Collaborative Spiral CT-working group, adapted from the National Cancer Institutes Cancer Data Standards Registry, the recommended smoking measures of the Behavior Change Consortium of the U.S. National Institutes of Health, and from Pistelli et al.1,2,3 The most important questions were: “When you last smoked every day, on average, how many cigarettes (shag) do/did you smoke a day?” (<5, 5 to 10, 11 to 15, 16 to 20, 21 to 25, 26 to 30, 31 to 40, 41 to 50, 51 to 60, >60); “What is the total number of years you have smoked/smoke cigarettes or shag every day? Do not include any time you stayed off cigarettes or shag for 6 months or longer.” (0 to 5, 6 to 10, 11 to 15, 16 to 20, 21 to 25, 26 to 30, 31 to 35, 36 to 40, 41 to 45, 46 to 50, >50 years) and; “If you have quit smoking, how long has it been since you quit?” (<1 month, 1 to 6 months, 7 months to 1 year, 1 to 3 years, 3 to 5 years, 6 to 10 years, 11 to 15 years, 16 to 20 years, >20 years, not applicable). The questionnaire was accompanied by brief information about the trial.
During this first recruitment phase, 106,931 of the 335,441 subjects (32%) who received the first NELSON questionnaire responded. Mean age of the respondents was 61 (standard deviation: 6.8 years). Response rates were lower in Belgium where we approached more women than in the Netherlands, but were overall equally distributed over the age categories (Table 17.1). Table 17.2 shows the number of respondents for each level of smoking duration, the number of cigarettes smoked per day, and the duration of smoking cessation. Nearly one third of the 106,931 respondents (33,909 [32%]) never smoked, 26,733 (25%) has been smoking for less than 20 years, and 24,783 (23%) quit smoking for more than 20 years.
Selection of Potential Participants In the Netherlands, at present, 23% of women smoke compared to 32% of men.4 In the past, this difference was greater when even fewer women and more men smoked. Therefore, fewer women in the Dutch population have accrued a long-term exposure to cigarettes compared to men. Because of the lower fraction of high-risk subjects among women, we anticipated before start of the trial that recruiting an equal number of high-risk women and men would require an enormous effort. Therefore, the Dutch Health Council and the Ministry of Health agreed to invite first men and only in the second phase also women. In that way, we would still be able to demonstrate possible differences in lung cancer detection between men and women, and at the same time limit our recruitment efforts.
FIGURE 17.1 The different steps in the recruitment process of the Dutch-Belgian helical CT lung cancer screening trial (NELSON) and the different time point at which quality of life will be assessed. CT, computed tomography; QOL, quality of life.
Because the smoking exposure history of all respondents on the first NELSON questionnaire was available, a careful decision could be made on whom to invite for the trial. First, the estimated lung cancer mortality risk of the respondents was determined. Next, the required sample size to show a mortality benefit of screening of 20%, 25%, and 30%, and the corresponding number of eligible subjects was determined for various selection scenarios, and finally, the required participationrate was determined, defined as the required response of eligible subjects to reach the required sample size. In the optimal selection scenario, the required participation rate was as low as possible, and the required sample size was within the ranges of our capacity in the Netherlands and Belgium (± 16,000 participants).
Our estimates of lung cancer mortality were based on the U.S. Cancer Prevention Study II (CPS II), a cohort study that started in 1982 and followed 508,579 men and 676,527 women, aged 30 years or older for 6 years.5 The CPS II reports lung cancer mortality rates per 100,000 person-years (PY) for groups of men with attained ages 50 to 79 (50 to 59, 60 to 69, and 70 to 79 years), smoking duration of 20 years or more (20 to 29, 30 to 39, 40 to 49, and ≥50 years), and one or more cigarettes smoked per day (1 to 19, 20, 21 to 39, 40, and ≥41 cigarettes per day). Because the CPS II monograph included only data on current smokers, the U.S. Cancer Prevention Study I (CPS I) was used to estimate the effect of smoking cessation. This prospective cohort study started following up 456,491 men and 594,551 women older than 30 years on July 1, 1960. Follow-up was a maximum of 12 years.6 By varying the thresholds for duration of smoking, the duration of smoking cessation, and the number of cigarettes smoked per day, the mean-estimated expected lung cancer mortality rate (per 1000 PY) for various selection scenarios was determined. Based on the most optimal selection scenario, current and former smokers with 10 years or less of cessation, who smoked more than 15 cigarettes a day for more than 25 years or 10 cigarettes a day for more than 30 years, were selected.7 Persons with a moderate or bad self-reported health who were unable to climb two flights of stairs and persons with a body weight greater than or equal to 140 kg were excluded from participation. Lung cancer patients diagnosed less than 5 years ago, subjects symptomatic for lung cancer, and persons who had a chest-CT examination less than 1 year before they filled in the first NELSON questionnaire were excluded as well.
TABLE 17.1 Characteristics of 335,441 Persons Who Received the First NELSON Questionnaire (First Recruitment) and Characteristics of the 106,931 Respondents
* Only in Belgium women were approached in the first recruitment round. † †The population registries of some communities in Belgium did not supply us with data on gender and/or birth date, and gender was not asked in our first questionnaire. ‡ ‡Age at mean date of response, which was October 1, 2003. * §Total also includes 69 subjects who responded, but returned a blank questionnaire.
From van Iersel CA, de Koning HJ, Draisma G, et al. Risk-based selection from the general population in a screening trial: selection criteria, recruitment, and power for the Dutch-Belgian randomised lung cancer multi-slice CT screening trial (NELSON). Int J Cancer 2007;120:868-874.
Power and Required Sample Size The required sample sizes to demonstrate a lung cancer mortality reduction of 20%, 25%, or 30% were calculated for the various selection scenarios. A 1:1 randomization, a power of 80%, a one-sided α-significance level of 0.05, 95% compliance in the screen group, 5% contamination rate in the control group, and 10 years of follow-up after randomization were assumed.8 With a power of 80%, enrolment of 17,300 subjects in NELSON is required to demonstrate a lung cancer mortality reduction of 25% or more and 27,900 subjects to demonstrate a lung cancer mortality reduction of 20% or more 10 years of follow-up. In Denmark, 4100 men and women, current and former smokers (quit < 10 years), aged 50 to 70, with at least 20 pack-years of smoking have been recruited through the public media. It is planned to pool mortality data with the Danish trial, so that the total number of participants in the NELSON trial will be more than 20,000. NELSON will then be the only trial without screening in controls that is expected to have an 80% power to show a lung cancer mortality reduction of at least 25% 10 years after randomization. When pooling with the Danish trial data, the fraction of women, which comprises 45% of all Danish trial participants, will also increase.
Our population-based recruitment gave insight in the risk profiles of the general population and we estimated that about 15% to 25% of the general (Dutch) population, age 50 to 75 would be the target for routine screening if our eligibility criteria would be applied. We, therefore, believe that our results are generalizable to a sufficiently large part of our population. Another advantage of a population-based recruitment approach is that it is less likely that potential participants exaggerated their smoking history to increase their chance to be invited for the trial, because they were unaware of the selection criteria.
TABLE 17.2 Number of Current smokers and Former Smokers (n = 73,022) of Total Respondents (106,931) on the First NELSON Questionnaire, Grouped by Smoking History (Ages 50-75)*
Number of Respondents, n
Cigarettes per Day
Smoking Duration (yrs)
Duration of Cessation
Total of Every Smokers(%)
Current Smokers
1 mo-5 yrs
6-10 yrs
11-15 yrs
16-20 yrs
>20 yrs
1-20
0-20
1718
949
753
1294
2153
14,562
21,429 (29%)
21-30
1865
1176
1299
1740
1420
3246
10,746 (15%)
31-40
5426
2268
1347
1173
701
935
11,850 (16%)
41-50
3683
1260
599
383
145
183
6253 (9%)
≥51
64
14
0
0
0
0
78 (0.1%)
21-40
0-20
208
152
131
338
639
3164
4632 (6%)
21-30
572
469
643
957
707
1384
4732 (6%)
31-40
3035
1445
928
720
366
394
6888 (9%)
41-50
1978
809
329
239
84
77
3516 (5%)
≥51
37
10
3
0
0
1
51 (0.1%)
≥41
0-20
27
29
22
39
91
464
672 (1%)
21-30
61
67
93
131
120
259
731 (1%)
31-40
260
188
148
132
70
96
894 (1%)
41-50
236
126
91
51
20
18
542 (1%)
≥51
5
1
0
2
0
0
8 (0.01%)
Total
Total of every smokers (%)
19,175 (26%)
8963 (12%)
6386 (9%)
7199 (10%)
6516 (9%)
24,783 (34%)
73,022 (100%)
*Numbers also include respondents who later appeared to be ineligible for participation for reasons other than smoking history (exclusion criteria) (11%). From van Iersel CA, de Koning HJ, Draisma G, et al. Risk-based selection from the general population in a screening trial: selection criteria, recruitment, and power for the Dutch-Belgian randomised lung cancer multi-slice CT screening trial (NELSON). Int J Cancer 2007;120:868-874.
Only gold members can continue reading. Log In or Register to continue
Aug 25, 2016 | Posted by drzezo in CARDIOLOGY | Comments Off on Low-Dose Computed Tomography Screening: Experiences from the Randomized Population-Based Nelson Screening Trial