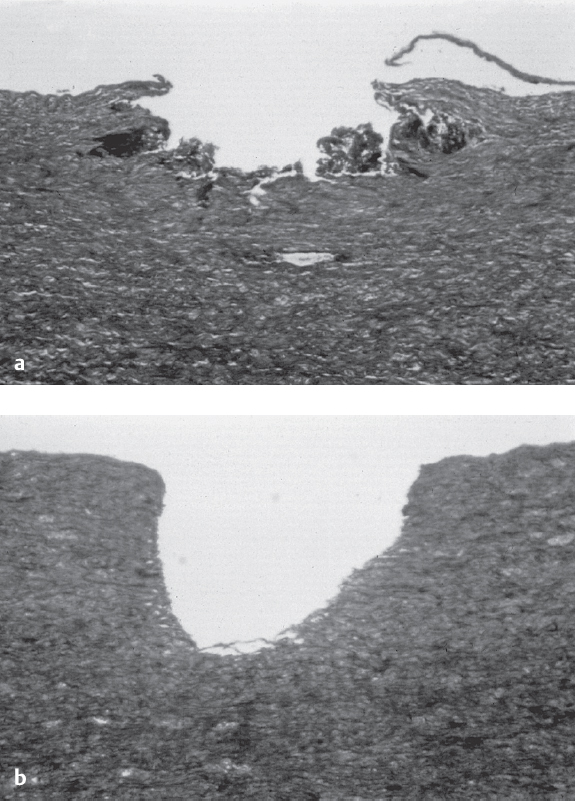
26 Laser Angioplasty Laser systems generate a coherent, parallel light beam of high energy density with a specific, uniform wavelength. The energy can be emitted continuously or pulsed. The energy density is inversely proportional to the wavelength of the emitted photons. Excimer laser. In current interventional cardiology the excimer laser using XeCl with a wavelength of 308 nm is established. A high-energy laser beam in the ultraviolet range is applied in pulsed form and causes ablation of the plaques by breaking chemical bonds with fragmentation of molecules on the surface (photochemical effect). As blood also absorbs ultraviolet radiation, direct contact of the laser catheter with the atheroma is required for ablation (contact laser). However, with high-energy laser irradiation there is also formation of vapor bubbles in the area of the catheter tip that leads to undirected barotraumatic damage of the vessel wall with the formation of dissections or vessel wall perforations. Contrast medium and blood increase the size of these generated vapor bubbles and correspondingly increase the traumatic energy generated. This effect can be suppressed by a continuous flush with normal saline during the laser irradiation. The introduction of the saline-flush technique was a significant advance in laser angioplasty that resulted in a marked reduction of dissections (Fig. 26.1). Due to the need for special equipment and the advances in alternative interventional techniques, the spectrum of indications is currently narrow. When considering an indication, the advantages and risks of laser angioplasty have to be weighed against those of other interventional modalities (e.g., stent, cutting balloon, rotational atherectomy). Laser systems are currently used for the following indications: Laser angioplasty is not indicated for: Laser catheter. Rapid-exchange catheters are predominantly used. The design of the catheter tip is shown in Fig. 26.3. At the proximal end there are connections to the laser system. Four catheter sizes are available: Table 26.1 Technical characteristics of a laser system (Spectranetics CVX300)
 Basics
Basics
 Indications and Contraindications
Indications and Contraindications
 Diffuse in-stent restenosis
Diffuse in-stent restenosis
 Long chronic occlusions (after wire crossing)
Long chronic occlusions (after wire crossing)
 Lesions with thrombus burden
Lesions with thrombus burden
 Bifurcation stenoses
Bifurcation stenoses
 Very eccentric stenoses
Very eccentric stenoses
 Stenoses in tortuous vessels
Stenoses in tortuous vessels
 Dissection
Dissection
 Instruments
Instruments
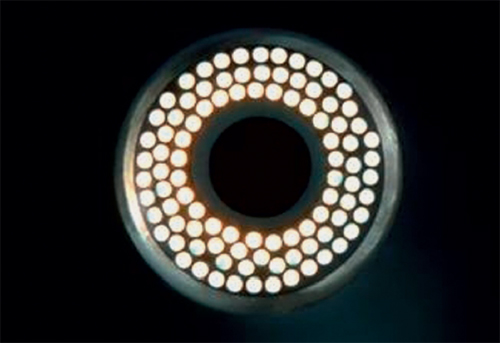
Excimer Laser System (Fig. 26.2, Table 26.1).

Active medium | XeCl, pulsed laser |
Wavelength | 308 nm UVB |
Pulse width | 125–200 nanoseconds |
Catheter output fluence | 30–80 mJ/mm2 |
Energy output | 200 mJ/pulse |
Repetition rate range | 25–40 Hz |
 0.9 mm with 65 fiberoptic bundles
0.9 mm with 65 fiberoptic bundles
 1.4 mm with 110 fiberoptic bundles
1.4 mm with 110 fiberoptic bundles
 1.7 mm with 140 fiberoptic bundles
1.7 mm with 140 fiberoptic bundles
 2.0 mm with 250 fiberoptic bundles
2.0 mm with 250 fiberoptic bundles
Protective glasses are required for all persons in the examination room. Otherwise, the standard instruments for conventional percutaneous coronary intervention (PCI) are required.
The working length of the system is 150 cm. The size of the guiding catheter (6F–9F) depends on the size of the laser catheter (Table. 26.2).
The guidewires used are stiff coronary guidewires (0.014 in.) of the “extra-support” type (length 190 or 300 cm). When using a special intracoronary guiding catheter, long wires are required (Fig. 26.4). Polymer-coated wires may not be used.
For chronic occlusions, recanalization wires (e.g., Confianza, Abbott Vascular, Temecula, CA, USA) are preferably used.