Chapter 42 Laparoscopic Aortic Surgery for Aneurysm and Occlusive Disease
Technique and Results
The initial enthusiasm of endovascular procedures to safely exclude abdominal aortic aneurysms is currently reduced because of the significant late failure rate, aneurysm rupture, and costs. With the improved technology, described laparoscopic techniques can be a durable alternative.1–3
Total laparoscopic aortic surgery in patients with occlusive disease can be performed routinely in the majority of patients.1 Since the first total laparoscopic aortic operation, the technique has been refined and can now be used in a patient with an aortic aneurysm.2,3
Technique
All patients receive the standard preoperative examination required for major aortic surgery. If necessary, coronary angiography and pulmonary function tests are performed. A laxative is given 1 day before the procedure like in bowel surgery. The patient is placed on the operating table on a vacuum bag. When tilting the table to the right, the patient can be positioned almost 70 degrees on the right side (Figure 42-1A). The left hemicolon and the splenic flexure are mobilized medially.
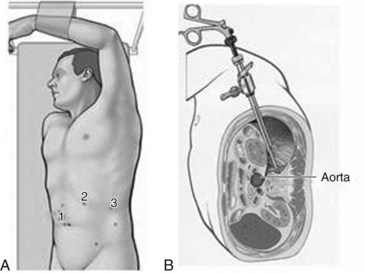
The technique of medial mobilization was originally described by Dion and colleagues3,4 to separate the abdominal contents from the retroperitoneal space. One laparoscopic retractor is required in obese patients. A left hemicolon retrorenal approach with medial mobilization of the left kidney and the ureter is usually preferred (see Figure 42-1B); this permits expeditious exposure of the aorta even in obese patients. This approach can also be used for medial viscero rotation to obtain access to the suprarenal aorta. All three surgeons are standing on the right side of the patient during the entire procedure.
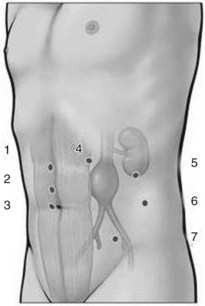
Laparoscopic exposure of the aorta is initiated at the level of the neck of the aneurysm.3 The left renal vein is one of the first structures we see when dissection is started. The laparoscopic camera stays in port 2 most of the time during exposure of the aorta (Figure 42-2). Especially in patients with occlusive disease, only the site for the anastomosis proximal to the origin of the inferior mesenteric artery is dissected. This exposure technique avoids damage of the lumbosacral nerves adjacent to the aortic bifurcation. During retroperitoneal dissection, the first assistant holds the camera and helps to put the tissue on attention with a grasping clamp (see Figure 42-2).
Lumbar arteries are controlled extra luminally from the left side. When the left-sided lumbar arteries are divided after clipping, the adjacent right-sided lumbar artery can be clipped. Lumbar arteries that are still bleeding after incision of the sac of the aneurysm are stitched with laparoscopic sutures and secured with a titanium clip to save time.5
Laparoscopic Anastomosis
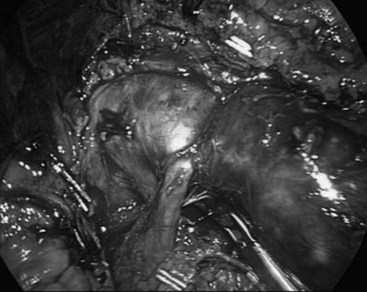
Laparoscopic dissection and suturing is performed with the surgeon standing on the right side of the patient5 (Figure 42-3). The transperitoneal left retrorenal exposure of the aorta permits access to the entire suprarenal aorta, permitting subdiaphragmatic cross-clamping (Figure 42-4). In patients with an end–end anastomosis with the proximal aorta, the posterior wall of the aorta is left intact as in open surgery.

< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


