Fig. 1.1
Chest wall injuries with multiple rib fractures and a flail segment are typically the result of severe, crushing-type injuries. This worker was crushed in the wheel well of a large transport truck and sustained multiple injuries including a flail chest, multiple extremity fractures, and a severe, degloving arm injury that resulted in below-elbow amputation (Photograph provided by, and used with permission of, the patient)
The term “flail chest” has typically been used to describe a biomechanically unstable chest wall following a traumatic injury. This results in a pathological degree of instability such that normal respiratory mechanics are interfered with: paradoxical respiration is often the result. This occurs during normal inspiratory effort, when, as a negative intrathoracic pressure is produced, the unstable chest wall collapses or caves in, rather than expands (Fig. 1.2). This compromises respiratory function and gas exchange. There is no generally accepted standard definition of a flail chest: it ranges from a minimum of two segmental fractures of adjacent ribs to as many as four segmental fractures of adjacent ribs [5–7]. For the purposes of defining this injury for research, clinical trials, and other studies, we have used the following definition of flail chest:
Fig. 1.2
An illustration of paradoxical respiration, which can occur as a result of chest wall instability: this is a common complication of a flail chest injury
≥3 unilateral segmental rib fractures
≥3 bilateral rib fractures
≥3 unilateral fractures combined with sternum fracture/dissociation
Note: At least three of the rib fractures involved in the flail segment must demonstrate displacement.
It is very difficult to break a bony ring (such as the pelvic ring or the rib cage) at only one spot; therefore, most fractures of a circular bony structure tend to occur at two sites. This is also the case for rib fractures. Although a number of different fracture patterns can be seen, typically, one fracture site is displaced and the rib “hinges” or deforms without translational displacement at the other site. This is important clinically, as often only the displaced fracture site needs to be reduced and stabilized: this corrects the angular deformity at the “hinge” site, which is intrinsically stable. This is discussed further in Chaps. 6 and 9 and is a principle by which unnecessary dissection can be avoided. Of course, if both fractures are displaced and unstable, they must both be stabilized [8]. The sternum may represent a separate site of injury and produces the same biomechanical effect as a displaced rib fracture. Fortunately, there is abundant experience with sternal fixation in the cardiac surgery realm, and specialized plates and instruments are available. Additionally, a number of other patterns can have a similar negative clinical effect as a standard flail chest and may represent operative indications, including:
Severe (100 %) displacement of three or more ribs
Marked loss thoracic volume/caved in chest (>25 % volume loss in involved lobe(s))
Overriding of three or more rib fractures (by minimum 15 mm each)
Three or more rib fractures associated with intraparenchymal injury—i.e., fractured rib embedded in the lung parenchyma
The traumatic force delivered to the chest wall in an injury of this nature typically produces instability and deformity, which has both short-term and long-term consequences for the patient [9–11]. This deformity can be static or fixed, as demonstrated in the computerized tomography (CT) scan depicted in Fig. 1.3, with severe, fixed loss of chest wall contour, loss of thoracic cage volume, and subsequent interference with respiratory function. It must be remembered that the chest wall and rib cage are in constant motion during the ventilatory process, and associated deformity or instability can be dynamic in nature. In some cases, when static deformity may not be severe, the primary manifestation of chest wall instability can be incapacitating pain for the patient. In this situation, it may be difficult or impossible to wean a patient from mechanical ventilation. Mechanical instability of the chest wall can result in severe pain, the requirement for heavy sedation and analgesia, resultant respiratory depression, poor respiratory toilet, and a progressive downward spiral of prolonged mechanical ventilation and the potential complications therein. An example is demonstrated in Fig. 1.4, depicting a young patient with severe chest wall pain following a left-sided chest wall injury. Reduction and fixation of the patient’s rib fractures resulted in an immediate decrease in narcotic medication requirement and rapid weaning and extubation. There is increasing evidence that this type of early primary fixation of multiple rib fractures may be superior to nonoperative treatment [12–15].
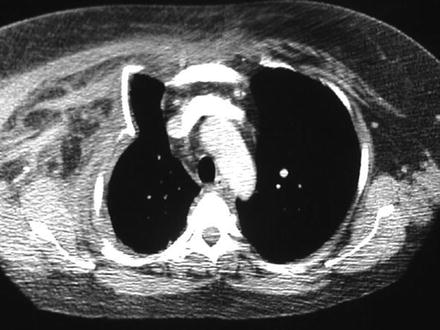
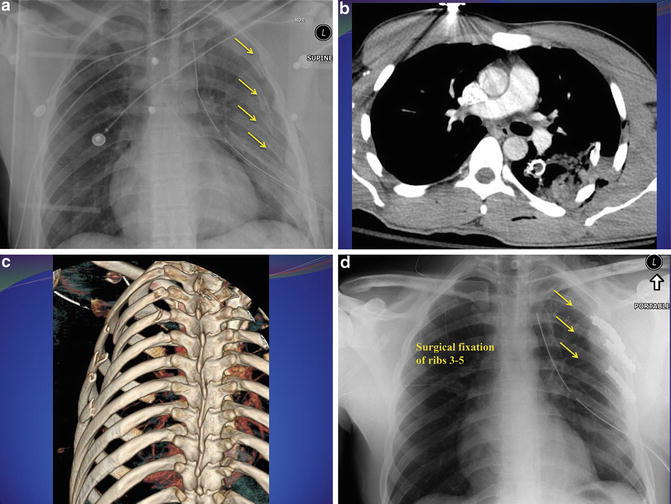
Fig. 1.3
A CT scan of a polytrauma patient with a severe right-sided chest injury, a flail segment, significant intrusion of the chest wall, and subsequent severe compromise of the thoracic cavity and respiratory function. This patient represents, with the current level of knowledge regarding these injuries, an ideal opportunity for surgical intervention. Reduction of deformity and stabilization in the reduced position has a number of theoretical and practical advantages
Fig. 1.4
(a) A 27-year-old man was accidentally crushed in a garbage compactor. This resulted in multiple, segmental left-sided rib fractures (ribs 3, 4, 5, 6) as seen on the initial trauma-room chest radiograph (yellow arrows). The patient had intractable pain, subsequently developed respiratory failure, and required prolonged intubation. (b) A CT scan demonstrated significant displacement of the rib fractures with intraparenchymal penetration of the fractured rib into the ipsilateral lung. (c) Three-dimensional reconstruction of the CT scan provides excellent representations of the nature and location of the fractures that can aid significantly in preoperative planning regarding surgical approach and tactics. This has become an integral part of the preoperative imaging of flail chest injuries. (d) A left thoracotomy, extrication of the ribs from the lung, rib fracture reduction, and fixation with 3.5 mm (unlocked) pelvic reconstruction plates were performed (yellow arrows). It is not always necessary to repair every rib fracture in a flail chest: the surgical goal is to stabilize the flail segment sufficiently to restore chest respiratory function without pathological deformation. The patient had immediate clinical improvement, a dramatic decrease in analgesic requirements, and was rapidly extubated
Associated Injuries
Most patients with a traumatic flail chest will have associated injuries, and these can be life threatening. While these injuries are discussed in detail in Chap. 10 (associated intrathoracic injuries) and Chap. 15 (associated fractures), it is important to emphasize that the presence of a flail chest should immediately prompt the initiation of the Advanced Trauma Life Support (ATLS) guidelines in the care of the patient. Associated injuries in this setting can be immediately fatal if not promptly treated. The flail chest patient depicted in Fig. 1.5 had sustained severe right-sided thoracic trauma with multiple segmental fractures of ribs 4 through 9, a tension pneumothorax, and rapid clinical deterioration. Rapid insertion of a chest tube resulted in decompression of the chest cavity and immediate clinical improvement: this case demonstrates the importance of detecting and treating other severe injuries prior to focusing on rib or sternal fractures. Additionally, injuries to the lung parenchyma or other intrathoracic structures are common and may dictate treatment initially (see Chap. 10).
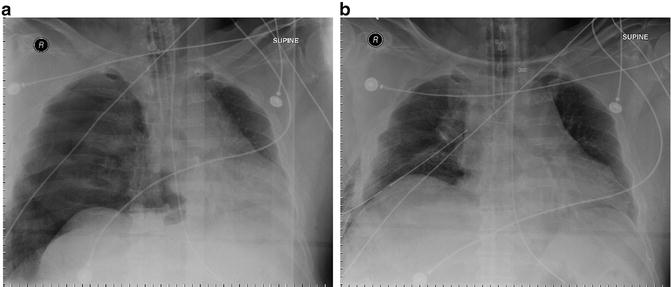
Fig. 1.5




(a) Initial chest radiograph of a polytrauma patient who was “T-boned” in a motor vehicle collision and sustained severe right chest wall trauma with multiple segmental fractures of ribs 4 through 9. The patient was intubated in the prehospital setting for respiratory compromise and, upon arrival to the trauma bay, rapidly deteriorated from a cardiovascular standpoint. The chest radiograph taken immediately upon arrival as part of the trauma protocol demonstrated a tension pneumothorax with severe deviation of the mediastinal structures and trachea. It could be argued that a chest radiograph of this nature should never be seen: the dire clinical situation combined with the physical examination of the chest would warrant immediate chest decompression with needle insertion or right-sided tube thoracostomy. (b) Following needle decompression, a large-bore chest tube was inserted with immediate improvement in cardiovascular parameters. This case demonstrates the importance of careful assessment of a flail chest patient for associated (potentially life-threatening) injuries
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
