Intralobar Sequestration
Presentation
You are consulted to evaluate a patient who presents to the oncology service. The patient is a 37-year-old woman with a history of leukemia. She completed her treatment regimen 1 month before her admission. During the past 3 weeks, she has been experiencing low-grade fever and a cough that is productive of mostly clear phlegm. On admission, a chest x-ray is obtained, and the patient is treated with broad-spectrum antibiotics for a presumed pneumonia. Blood and sputum cultures are negative for bacteria and fungi.
▪ Chest X-rays
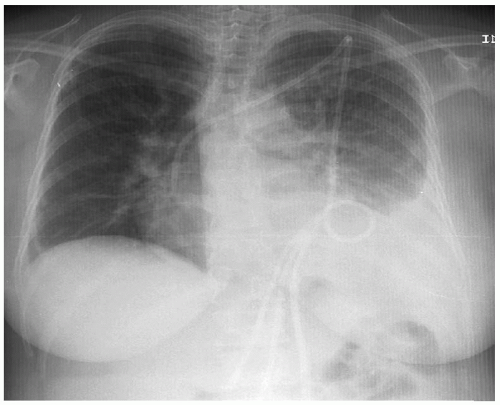 Figure 40-1 |
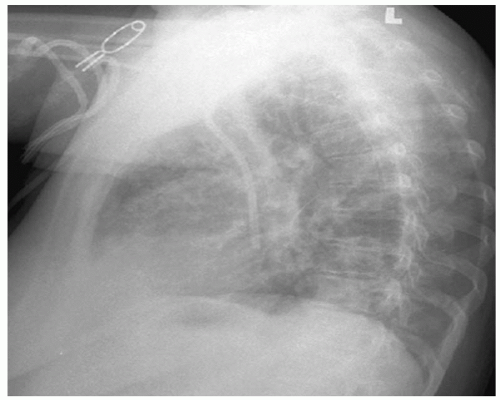 Figure 40-2 |
Chest X-ray Report
The chest x-rays demonstrate a consolidation of the left lower lobe obscuring the left heart border and left hemidiaphragm. The tip of the central venous catheter is in the right atrium. ▪
Discussion
The patient is postchemotherapy and is exhibiting signs, symptoms, and chest x-ray evidence of a pulmonary infection. Blood and sputum studies have not revealed any organisms, and sputum production has been scant despite the chest x-ray findings.
Recommendation
Flexible fiberoptic bronchoscopy.
Case Continued
Flexible fiberoptic bronchoscopy reveals left lower lobe bronchial erythema and minimal acute inflammation of the posterior segmental bronchus. Scanty secretions are present. Bronchial washings reveal many leukocytes and no bacteria. Cultures from the bronchoscopy specimen recover Aspergillus species. Further evaluation of the patient reveals a past history of recurrent chest infections. Repeat chest x-rays do not indicate improvement from the initial admission x-ray. The patient continues to have low-grade fever on broad-spectrum antibiotics.
Recommendation
The patient’s clinical scenario is consistent with that of a left lower lobe fungal infection with possible cavitation. The extent of radiographic lung disease prompts further diagnostic evaluation. Although there is no evidence of a lung abscess on the chest x-ray, computed tomography (CT) scans of the chest provide a better anatomic definition of the inflammatory process.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


