A 43-year-old man with a prosthetic aortic valve used illicit drugs intravenously and came to the hospital with infective endocarditis. Several days later, pauses were noted on his electrocardiographic monitoring strips ( Figure 1 ).
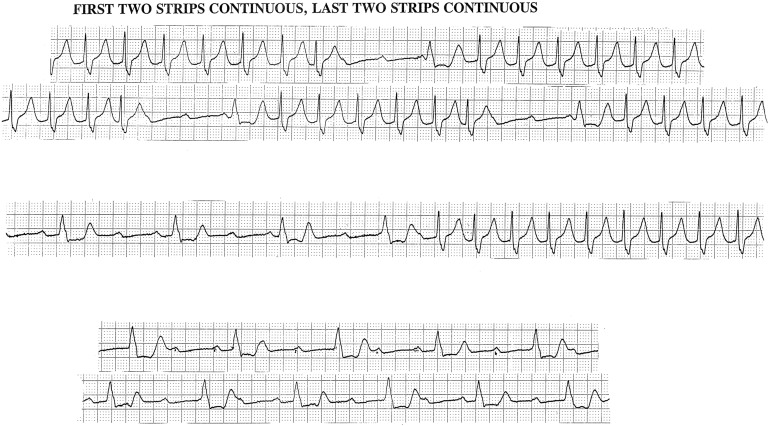
The atrial rhythm was sinus arrhythmia and tachycardia at a rate of 107 beats/min. Runs of 1:1 atrioventricular (AV) conduction with a long PR interval (P waves were buried in the preceding T waves) and right bundle branch block (BBB) were interrupted by periods of complete AV block and the emergence of an idioventricular pacemaker that showed the warm-up phenomenon. The complete AV block probably resulted from persistent right BBB with intermittent left BBB.
The development of any degree of AV block in a patient with infective endocarditis on a left-sided valve, and especially on a prosthetic aortic valve, suggests a perivalvular abscess impinging on the conduction system, usually below the AV node. It is an ominous sign because the degree of AV block usually worsens requiring electronic cardiac pacing, replacement of the aortic valve, and drainage of the abscess. The pacemaker and the new valve are both at risk to become infected despite antibiotics. Even when they remain infection free, the patient may not remain free of drugs.
Disclosures
The authors have no conflicts of interest to disclose.
See page 1855 for disclosure information.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


