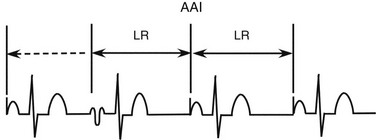
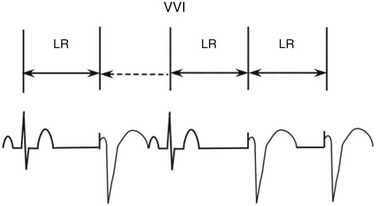
117 Since the first epicardial pacing system was implanted in 1958, pacemaker technology has evolved rapidly. Sophistication of sensing circuitry led to the introduction of single-chamber demand pacing systems in 1963. Although atrial-synchronous systems and dual-chamber systems were described in the 1950s, clinical use of such devices did not occur for many years. In the 1970s, lithium batteries and programmability were introduced. Milestones of the 1980s include greater acceptance of dual-chamber pacing systems and the introduction of rate-adaptive pacing systems. The 1990s and the 2000s witnessed the introduction of advanced sensor technology, new pacemaker algorithms, and enhanced automaticity of many programmable features. The use of pacing has increased significantly from 46.7/100,000 in 1993 to 61.6/100,000 in 2009, with the percentage of dual chamber devices increasing from 62% to 82% during this period.1 Since the first introduction of a three-letter code describing basic pacemaker functions in 1974, the code has been updated periodically by a committee comprising members of the North American Society of Pacing and Electrophysiology (NASPE) and the British Pacing and Electrophysiology Group (BPEG). The most recent code consists of five letters (Box 117-1). The first position indicates the chamber or chambers that are stimulated: A (atrium), V (ventricle), or D (dual chamber, both A and V). The second position indicates the chamber or chambers in which sensing occurs: A (atrium), V (ventricle), or D (dual chamber, both A and V). The third position indicates the function: I (inhibition), T (triggered), or D (a dual function of atrial tracking and ventricular inhibition). The fourth position of the code indicates that rate modulation is present by the letter R. Rate modulation is the use of a sensor to meet the patient’s metabolic demands, independent of intrinsic cardiac activity. The fifth position indicates whether multisite pacing is present: A (atrium), V (ventricle), or D (both A and V). Multisite pacing is defined as more than one stimulation site in any single chamber. In any of the positions, O indicates that pacing, sensing, or a function is not present. Criteria established by a joint committee of the American College of Cardiology, the American Heart Association, and the Heart Rhythm Society have categorized indications for pacing as class I, generally indicated; class II, possibly indicated; and class III, not indicated.2 Class II has been divided into class IIa for recommendations for which there is general agreement and class IIb for which there is some disagreement. The evidence supporting the recommendations are ranked. The weight of evidence is ranked A if there are multiple randomized trials involving a large number of subjects and B if data were derived from a limited number of trials involving a relatively small number of subjects. The weight of evidence is ranked C if expert consensus is the primary source of the recommendation.2 Although some indications for permanent pacing are relatively certain or unambiguous, others require considerable expertise and judgment. The clinician prescribing permanent pacing systems should be aware of the indications and controversies regarding indications. Acquired atrioventricular (AV) block is most commonly idiopathic and related to aging, but the potential causes are many. Class I indications for permanent pacing in patients with acquired AV block include any AV block with associated symptoms, as well as AV block after AV node ablation or persistent AV block after cardiac surgery. For some patients, heart failure is a manifestation of AV block. In addition, some patients require medications that can cause symptomatic bradycardia and might need pacing. For postoperative AV block, the guidelines do not specify a period to wait postoperatively for recovery of conduction. Class I indications also include acquired AV block below the level of the AV node or associated with marked pauses, such as longer than 3 seconds, or a ventricular escape rate less than 40 beats/min. Because the cardiovascular risk is believed to be particularly high in patients with second- or third-degree block and specific underlying conditions, permanent pacing is indicated in these patients even in the absence of symptoms. These conditions include neuromuscular diseases such as myotonic dystrophy, Kearns-Sayre syndrome, peroneal muscular atrophy, and Erb limb girdle dystrophy. Myotonic dystrophy has been associated with an increased risk of sudden death believed to be caused by progressive conduction system disease.3 Exercise-related AV block is also an indication for pacing. Advanced second-degree AV block or alternating bundle branch block in the setting of bifascicular block is considered a class I indication. Asymptomatic type II second-degree AV block with a wide QRS is a class I indication. Transient, infranodal, high-grade AV block and associated bundle branch block is a class I indication.2 Class IIa indications include asymptomatic type II second-degree AV block with a narrow QRS complex, and asymptomatic second-degree AV block at intra-His or infra-His levels based on electrophysiological testing.2 First-degree or second-degree AV block with hemodynamic compromise is also considered a class IIa indication, because some patients develop pacemaker-like syndrome as a result of conduction delay. In patients with bifascicular block, asymptomatic severe prolongation of the His-ventricle interval (>100 ms), asymptomatic pacing-induced infra-His block that is not physiological, or syncope when other causes such as ventricular tachycardia have been excluded are considered class IIa indications for pacing. First-degree AV block in patients with neuromuscular disorders is considered a class IIb indication because the risk of progression to AV block is high. Another class IIb indication includes AV block that might have occurred because of drug use or toxicity, but there is a risk of recurrence of AV block. First-degree AV block in a patient with left ventricular dysfunction and congestive heart failure in whom hemodynamic improvement with AV interval optimization can be demonstrated is a class IIb indication.2 Asymptomatic and persistent second- or third-degree block at the AV node level is a class IIb indication.2 Symptomatic congenital complete AV block remains a class I indication for pacing in pediatric patients.2 In addition, in pediatric patients with congenital complete AV block, the presence of a wide QRS escape rhythm, ventricular dysfunction, or complex ventricular ectopy is also a class I indication. In pediatric patients, an average heart rate less than 50 beats/min, pauses two to three times the basic cycle length, or symptoms associated with chronotropic incompetence are considered class IIa indications. In pediatric and adult patients with adequate rate, narrow QRS complex, and normal ventricular function, pacing is a class IIb indication. For adult patients with congenital complete AV block, the timing and indications for permanent pacing are more controversial and continue to evolve.4 As a result of data regarding the high incidence of unexpected syncope in adult patients with congenital complete AV block, prophylactic pacemaker implantation is often considered.2,4 Sinus node dysfunction may be manifested by abrupt sinus pauses or gradual sinus slowing. Symptomatic chronotropic incompetence and symptomatic sinus bradycardia occurring spontaneously or as the result of drug therapy are considered class I indications for pacing. In patients with minimal or no symptoms and chronic heart rates less than 40 beats/min, pacing is a class IIb indication.2 Neurocardiogenic syncope typically has both cardioinhibitory and vasodepressor components. Pacing during most episodes of neurocardiogenic syncope is still associated with a significant fall in blood pressure and symptoms because of the continued vasodepressor response. Therefore, even in the presence of significant bradycardia, pacing is usually not considered first-line therapy. A number of randomized trials have failed to show a substantial benefit in increasing the freedom from recurrent syncope.5,6 As a result, neurocardiogenic syncope with documented bradycardia is considered a class IIb indication for pacing; however, there are some recent studies that indicate a selective use of pacing.7,8 In the Third International Study on Syncope of Uncertain Etiology (ISSUE-3) trial, in patients 40 years or older with at least three syncope episodes in 2 years, and with documentation of syncope with 3 seconds or more of asystole or 6 seconds or more of asystole without syncope, 77 patients were randomized to dual-chamber pacing on or off with an algorithm to increase the pacing rate with a sudden decrease in heart rate. The syncope recurrence rate was 57% in the “pacing off” group and 25% in the “pacing on” group (P = 0.039).7 When pacing is performed in this setting, dual-chamber pacing is necessary to preserve the atrial contribution to cardiac output. Modifications to the pacing strategy are being studied to make dual chamber pacing more effective in ameliorating neurocardiogenic syncope. The heart rate can be adjusted according to measured changes in impedance to estimate myocardial contractility, using so-called closed loop stimulation. Although retrospective data suggest that this approach may reduce the frequency of recurrence of syncope, additional prospective studies are needed.8 In patients with syncope of unknown origin, a randomized, multicenter study examined patients exhibiting a pause of 10 seconds or more when given an intravenous bolus of 20 mg adenosine triphosphate. These patients were randomized to atrial inhibited (AAI; 30 beats/min) or DDD pacing (70 beats/min). In the DDD pacing group, 21% of patients had recurrence of syncope compared to 66% of patients in the AAI group. Of note, the mean age in these studies was 76 years of age.9 Carotid sinus hypersensitivity has been shown to be a cause of syncope, particularly in the elderly. However, because an abnormal response can occur even in asymptomatic persons, caution must be used when spontaneous bradycardia has not been demonstrated. In cases in which syncope has occurred during carotid sinus stimulation and carotid sinus pressure has resulted in pauses of 3 seconds or more, a class I indication is present. If such an abnormal carotid sinus pressure response is obtained but syncope did not occur in circumstances suggesting carotid sinus stimulation, a class IIa indication is present. In addition, there may be a role for pacing in patients with unexplained falls and evidence of carotid sinus hypersensitivity. Recent studies do not show a difference in the recurrence of events in patients pacing on treatment using ventricular inhibited (VVI), DDDR, or DDDR with sudden bradycardia response.10 Numerous studies have examined various pacing algorithms to prevent atrial fibrillation. Most of these algorithms involve increasing the pacing rate to suppress atrial ectopy that is believed to trigger atrial fibrillation. Whereas most randomized studies have not demonstrated a beneficial effect, some studies have suggested a modest decrease in the occurrence of atrial fibrillation. In the Study of Atrial Fibrillation (SAFARI) trial, patients with AF recorded were randomized to atrial fibrillation pacing prevention strategies. Overall, there was a small reduction in the occurrence of atrial fibrillation. In patients with a high burden of atrial fibrillation, the reduction in atrial fibrillation was greater.11 Pacing for atrial fibrillation reduction is a class III indication. Numerous randomized, controlled trials have demonstrated benefit of cardiac resynchronization therapy in improving symptoms and outcomes in patients with drug-refractory heart failure. Cardiac resynchronization therapy is the pacing of the left and right ventricles to improve the hemodynamics that are impaired because of bundle branch block. These randomized studies have shown improvement in New York Heart Association classes, 6-minute walk time, oxygen consumption, brain natriuretic peptide levels, neurohormonal levels, ejection fraction, end-diastolic and end-systolic dimension, heart failure hospitalizations, and all-cause mortality.12 The current indications for resynchronization therapy (class I) include QRS duration of 120 ms or greater, left ventricular ejection fraction of 35% or less, sinus rhythm, and class III or ambulatory class IV heart failure symptoms on optimal medical therapy. Because the largest randomized trial excluded patients with atrial fibrillation, the presence of atrial fibrillation results in classification as a class IIa indication.2,12 Early studies suggested that right ventricular apical pacing resulted in a significant reduction in outflow tract gradient and ameliorated symptoms. However, a subsequent randomized multicenter trial failed to demonstrate benefit in patients with pacing. A subset of elderly patients might have exhibited some improvement. An analysis from the Cochrane Database concluded that clinical trial data are inconclusive regarding an effect of pacing on outcome in this patient population.13 Therefore, pacing in medically refractory symptomatic patients with significant resting or provoked gradient owing to hypertrophic cardiomyopathy is a class IIb indication.2 These patients should be considered for a dual chamber ICD because of the risk of sudden death. In the ventricular inhibited (VVI) pacing mode, pacemaker output is inhibited by a sensed ventricular event (Figure 117-1). The lower rate interval determines the longest interval between any sensed or paced ventricular events. The interval from the previous sensed or paced ventricular event to the subsequent paced ventricular event is the lower rate interval. If the time interval from the last sensed ventricular event to the first paced ventricular beat is longer than the time interval between ventricular paced beats, ventricular hysteresis is present. Any ventricular event occurring after a paced or sensed ventricular event within the ventricular refractory period is not sensed and does not reset the timing cycle. Figure 117-1 In the ventricular inhibited (VVI) pacing, the lower rate interval (LR) is the time from the last intrinsic or paced ventricular event to a ventricular paced event. When the LR interval has been completed, a ventricular paced event will occur. If an intrinsic beat occurs before the LR is completed, the ventricular output will be inhibited. The first QRS complex is intrinsic, and after the LR interval is completed a second intrinsic beat has not occurred; therefore, the second QRS complex is a paced ventricular event. The third QRS complex is again intrinsic. Following the third QRS complex, intrinsic QRS complexes do not occur within the LR interval. Thus, the fourth and fifth QRS complexes are paced. The double-headed arrows indicate a full LR interval has transpired. The dotted single-headed arrow indicates that the full LR interval has not been completed and an intrinsic QRS complex inhibits ventricular pacing. Atrial inhibited (AAI) pacing incorporates the same timing cycles as VVI pacing, with the obvious difference that pacing and sensing occur in the atrium, and pacemaker output is inhibited by a sensed atrial event (Figure 117-2). An atrial paced or sensed event initiates a refractory period during which atrial events do not reset the timing cycle. Confusion can arise when multiple ventricular events occur during atrial pacing. For example, when the atrial timing cycle ends, an atrial pacing stimulus is delivered regardless of ventricular events, because an AAI pacemaker does not sense in the ventricle. If the ventricular signal is inappropriately sensed by the atrial lead (far-field sensing), the atrial timing cycle is reset. This abnormality can sometimes be corrected by making the atrial channel less sensitive or by lengthening the atrial refractory period so that a conducted ventricular complex is not sensed.
Implantable Pacemakers
History of Pacing
Pacemaker Nomenclature
Indications for Cardiac Pacing
Acquired Atrioventricular Block
Congenital Complete Heart Block
Sinus Node Dysfunction
Neurocardiogenic Syncope
Carotid Sinus Hypersensitivity
Pacing for Atrial Fibrillation
Resynchronization Therapy
Hypertrophic Cardiomyopathy
Basic Pacemaker Function and Modes
Ventricular Inhibited Pacing
Atrial Inhibited Pacing
Implantable Pacemakers