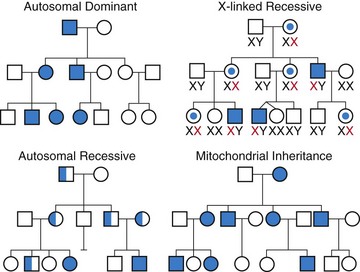
71 The four major modes of inheritance are summarized in Figure 71-1. In most cardiovascular genetic diseases, inheritance is autosomal dominant, whereby the disease can be expressed when the mutation is present in just one allele. As a result, the chance of passing on the gene mutation from parent to offspring is 50%. Most primary arrhythmogenic diseases and inherited cardiomyopathies are inherited in this fashion. The other three modes of inheritance, shown in Figure 71-1, are significantly less common. Autosomal recessive inheritance requires the person to inherit the mutation on both alleles for disease to develop (i.e., one mutation is inherited from each parent). The chance of passing on the gene mutation from parent to offspring is 25%. The Jervell-Lange-Nielsen form of familial long QT syndrome is inherited in an autosomal recessive fashion. X-linked inheritance refers to the situation whereby the gene mutation is located on the X-chromosome. In this case, males develop the phenotype, while females most often are asymptomatic gene mutation carriers. Rare forms of dilated cardiomyopathy have been shown to have an X-linked pattern of inheritance. Mitochondrial inheritance is a non-Mendelian pattern in which transmission of disease occurs exclusively via females; it involves inheritance of mutant mitochondrial DNA by offspring. Although uncommon, this form of inheritance is often seen in mitochondrial diseases that can clinically manifest with a hypertrophic cardiomyopathy phenotype (or phenocopy). Figure 71-1 The four most common modes of inheritance in cardiovascular genetic disease. Autosomal dominant inheritance accounts for more than 90% of cases of genetic heart diseases. Squares, Males; circles, females; open symbols, clinically unaffected; filled-in symbols, affected; spot in middle of symbol, obligate carrier; half-filled symbol, heterozygote gene carrier in an autosomal recessive family. Genetic testing is not a simple blood test. Many considerations arise with every family. A complete cardiogenetic evaluation is required, which includes confirming the clinical diagnosis in the proband, understanding the probabilistic nature of genetic testing and the need for genetic counseling, and taking a detailed family history to get a sense of disease penetrance and patterns of disease.1 In all patients and families with a genetic heart disease, genetic counseling is essential. Genetic testing options span all stages of life, from the preimplanted embryo or fetus, to children and adults. Appropriate pretest and posttest genetic counseling is a vital component of genetic testing. Apart from the diagnostic usefulness of genetic testing within families, a specific gene result may guide therapy and provide information about prognosis. The cardiac genetic counselor therefore plays a key role in the testing process, ensuring that the individual understands the clinical and psychosocial implications of every possible result and the limitations of the tests, including difficulties in interpretation of the results; and guiding discussion of other issues such as genetic testing of children, prenatal and preimplantation genetic diagnosis, and access to insurance.2
Genetic Testing
Basic Genetics
Modes of Inheritance
Genetic Testing in Cardiovascular Disease
General Principles
Genetic Counseling and Informed Consent
Genetic Testing



