Chapter 8 Hybrid Cardiac Imaging
INTRODUCTION (See Chapter 22)
The constant technological developments of noninvasive imaging over the past decades have contributed to the enhancement of our pathophysiologic understanding of many cardiac conditions. Particularly in coronary artery disease (CAD), management is based upon assessment of both the presence of coronary stenoses and their hemodynamic consequences.1,2 Hence, noninvasive imaging helps to guide therapeutic decisions by providing complementary information on coronary morphology and on myocardial perfusion and metabolism using different imaging tools,3,4 including nuclear techniques such as single-photon emission computed tomography (SPECT) or positron emission tomography (PET), computed tomography (CT) techniques such as electron beam CT (EBCT) and multislice CT (MSCT), or cardiac magnetic resonance (CMR).
Thus, the interest in hybrid imaging has rapidly spread onto cardiac applications and has changed the landscape of noninvasive cardiac imaging by bringing the different clinical specialties (i.e., cardiology, radiology, nuclear medicine) closer together.5 Additionally, it has driven the development and production of dedicated hybrid scanners in an effort to simplify image coregistration and improve patient throughput for specialized cardiac imaging centers. For the evaluation of a patient with heart disease, hybrid imaging introduces a multifaceted approach to cardiovascular assessment. This approach facilitates the detection and quantification of coronary atherosclerosis through the use of coronary artery calcium scores (CACS) and coronary angiography, the quantification of vascular reactivity and endothelial integrity, the identification of flow-limiting coronary stenoses, and the assessment of myocardial viability and metabolism by means of PET. Thus, by revealing the burden of anatomic CAD and its physiologic relevance, hybrid imaging can provide noninvasively unique information that may help to improve diagnosis and risk stratification and guide management decisions in CAD patients.
TECHNICAL CONSIDERATIONS OF HYBRID IMAGING
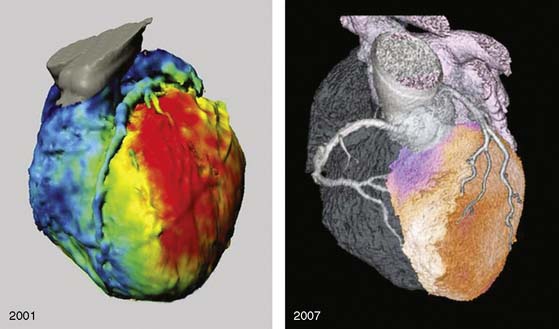
Several pioneering attempts of software-based image fusion from conventional coronary angiography (CA) and SPECT paved the way for hybrid imaging but were not implemented into clinical practice because their invasiveness precluded use for noninvasive preinterventional decision making.6–9 Fusion of CT and nuclear techniques for three-dimensional hybrid imaging was initially cumbersome, and the quality of the images suffered from several limitations (Fig. 8-1). The temporal and spatial resolution required for consistently good delineation of the coronary tree was not met by early 4- or 16-slice CT devices. Furthermore, the lack of dedicated cardiac fusion software rendered image processing tedious and time-consuming. Many new developments in hardware (e.g., 64-detector CT devices) and software (dedicated cardiac fusion software, high-powered postprocessing workstations) have helped to improve image quality and promote clinical availability of hybrid imaging (Fig. 8-2).
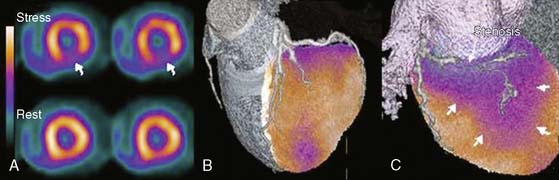
For cardiac applications, a three-dimensional display of the fused images (generated by volume-rendering technique)10 is preferable compared to oncologic or neurologic applications, because it allows the best evaluation of myocardial territories and their respective tributaries. Thus, an important prerequisite of hybrid imaging is accurate image coregistration. Misalignment may result in erroneous allocation of perfusion defects and coronary artery territories. From a computational perspective, image coregistration can be achieved by a software-based or hardware-based approach.11 Hardware-based image coregistration permits the acquisition of coregistered anatomic and functional images using hybrid scanners (such as PET/CT or SPECT/CT devices) with the capability to perform nuclear and CT image acquisition almost simultaneously, with the patient’s position fixed. Inherently, image fusion is performed fully or semiautomatically by superposition of image data sets. With software-based coregistration, image data sets can be obtained on standalone scanners and fused manually through the use of landmark-based coregistration techniques (Fig. 8-3). Intuitively, the hardware-based approach appears preferable, since manual coregistration may be hampered by issues of accuracy and user interaction. This is why, to date, hybrid PET/CT devices are widely used for whole-body PET/CT imaging, predominantly in oncology.
However, in contrast to whole-body PET/CT, the routine use of fully automated hardware-based image coregistration for cardiac hybrid applications is limited by organ-specific characteristics. Despite fixation of the patient’s position and orientation, minor beat-to-beat variations in the heart’s position may interfere with accurate image coregistration. Furthermore, CT image acquisition and analysis requires electrocardiographic gating, and images are generally reconstructed in mid-diastolic phases for obtaining optimal image quality.12 By contrast, for sufficient quality of the SPECT images, the nongated data set is used, resulting in a slight mismatch of ventricular size between CT and SPECT images. Finally, the position of the heart is highly susceptible to respiratory motion. The CT scan is performed during a single inspiratory breath hold, but SPECT images are acquired during normal breathing, without accounting for respiratory motion unless respiratory gating is used. In fact, whole-body PET/CT studies have shown significant misalignment of the heart between superimposed PET and CT acquired during inspiration.13,14
These factors contribute to the notion that despite the integration of high-end CT devices (with the capability to perform state-of-the-art coronary CT angiography) with nuclear scanners to form dedicated cardiac hybrid scanners, manual image coregistration may remain indispensable.15 Published reports with x-ray-based attenuation correction have taught us that automated coregistration of CT and SPECT images is often unreliable, and manual correction for misalignment is needed in the vast majority of cases.16,17 Dedicated cardiac fusion software packages are now commercially available, allowing software-based hybrid imaging with an excellent interobserver reproducibility and short processing durations (see Fig. 8-3). In a validation study using software-based SPECT/CT fusion from standalone scanners, reproducibility and feasibility of this method were evaluated by assessing cardiac surface landmarks in 15 patients with a single coronary stenosis and a single perfusion defect.18 The authors reported an excellent interobserver variability (r = 0.99; P < 0.0001) for landmark detection and reasonably short processing times of less than 15 minutes per patient. The full integration of these fusion software packages into the regular postprocessing applications for CT angiography will further minimize time expenditure and improve workflow for hybrid imaging (by avoiding repeat actions such as coronary artery tracking from CT angiography images).
HYBRID IMAGING: COMPREHENSIVE “ONE-STOP SHOP”
Atherosclerotic disease accounts for the majority of fatalities reported in industrialized countries. The diagnostic gold standard for establishing the presence of CAD is still x-ray coronary angiography, with all its drawbacks. A major limitation of this technique is its invasive nature, with considerable procedure-related morbidity (1.5%) and mortality (0.15%). In addition, the physiologic significance of any lesion is frequently difficult to assess from angiographic information alone. Furthermore, up to 75% of all invasive angiograms in the United States remain purely diagnostic, and between 20% and 40% of all diagnostic invasive coronary angiograms reveal no clinically significant disease,19 so noninvasive procedures have the potential to play an important role in the future by eliminating a substantial fraction of these invasive angiograms (e.g., in cases of atypical chest pain, equivocal stress test results, and low to intermediate clinical probability of coronary disease).
Multislice CT angiography has rapidly evolved from an experimental technique to the most promising imaging modality for the noninvasive visualization of coronary arteries. Using the latest generation of CT scanners (dual-source CT, 256 detectors and more), excellent image quality can be achieved in the vast majority of patients, with values for sensitivity, specificity, and positive and negative predictive values averaging 92%, 96%, 79%, and 99%, respectively.20 With its high negative predictive value, noninvasive angiography may play an important role when the clinical goal is to rule out CAD in patient populations with low clinical probability for CAD. Nonetheless, a minor drawback of CT angiography remains the moderate positive predictive value, insofar as stenoses tend to be overestimated owing to partial volume effects from coronary artery–wall calcifications and other image artifacts.
The value of hybrid imaging originates from the spatial correlation of structural and functional information on the fused images, which facilitates a comprehensive interpretation of coronary lesions and their pathophysiologic relevance. Although this can be achieved by mental integration, coronary artery anatomy may vary considerably, therefore standard myocardial distribution territories correspond in only 50% to 60% with the real anatomic coronary tree.7 First clinical results with noninvasive hybrid imaging were presented by Namdar and coworkers using fusion of myocardial perfusion PET with 13N-ammonia and 4-slice CT angiography in 25 patients with CAD. Sensitivity, specificity, and positive and negative predictive value of hybrid PET/CT for the detection of flow-limiting stenoses in the main coronary vessels were 90%, 98%, 82%, and 99%, respectively, compared to the clinical gold standard of PET and conventional coronary angiography. These encouraging results were confirmed by a similar study by Rispler and coworkers.21 The authors compared the diagnostic accuracy of hybrid SPECT/CT imaging for the detection of flow-limiting coronary artery stenoses with CT angiography alone in 56 patients with angina pectoris. Hybrid SPECT/CT resulted in a significant improvement in specificity (from 63% to 95%) and positive predictive value (from 31% to 77%) compared to CT alone, without any change in sensitivity and negative predictive value. A similar study by Santana and colleagues showed an improved diagnostic accuracy of hybrid SPECT/CT imaging compared to SPECT alone (P < 0.001) and to the side-by-side analysis of SPECT and CT (P = 0.007) for diagnosis of obstructive CAD on conventional coronary angiography.22 These data show that hybrid SPECT/CT imaging may play an important role in the noninvasive diagnosis of CAD as a decision-making tool for assessing the need for revascularization in coronary artery stenoses.
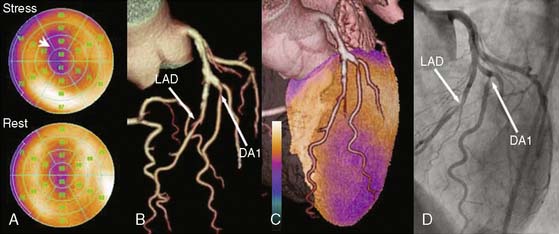
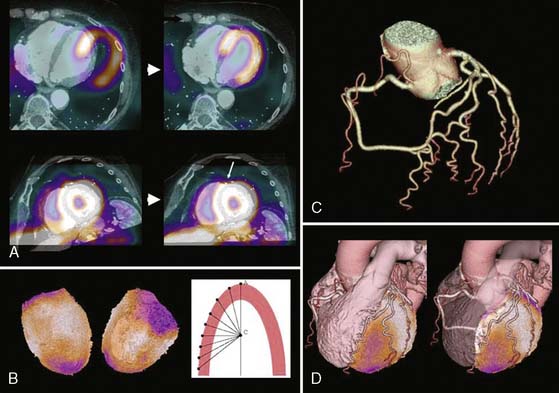
A recent publication focused on the role of hybrid SPECT/CT imaging for assessing the hemodynamic relevance of coronary artery stenoses and its potential added clinical value over side-by-side analysis in 38 high-risk patients with abnormal perfusion on SPECT (Fig. 8-4).3 The main clinical benefit of hybrid SPECT/CT imaging was a significant reduction in the number of coronary lesions with equivocal hemodynamic significance (from n = 40 to n = 16; P < 0.001) (Fig. 8-5). Added diagnostic information of SPECT/CT fusion was more commonly found in patients with stenoses of small vessels such as diagonal or posterolateral branches. Hence, the hybrid approach allows reliable allocation of perfusion defects to its subtending coronary artery, compared to the side-by-side analysis—a finding that might be particularly useful to guide revascularization strategies in symptomatic patients with multivessel disease and/or intermediate-degree stenoses.