Heart Attack
Half of all deaths are caused by disease of the heart and blood vessels. The chances are good, therefore, that you will be on hand when someone actually has a heart attack. It is a common occurrence. If the heart attack strikes on the golf course, by a fishing stream, on a ski slope, or at any place far from medical aid, what can you do? (After a lifetime of backpacking, fly-fishing, and skiing in remote areas I have a deep personal interest in this subject.)
There are only a few things that the nonmedical person can do for the victim of a heart attack. These few things, however, may be very important. There are also some things that you should not do.
A heart attack will be one of two things: (1) acute left heart failure or (2) some type of coronary artery syndrome.
Acute Left Heart Failure
The symptom of acute left heart failure will be shortness of breath. The victim will be panting very rapidly with shallow breaths, the color of his lips and earlobes may be bluish, he will refuse to lie down flat, and he will fight you if you try to force him to do so. He will be sitting up, gasping desperately for breath. He is fighting for breath because his lungs are engorged with blood, which is trapped in back of a failing left heart (Chap. 6).
What to Do
Place tourniquets as high up as you can around the patient’s arms and legs. The tourniquets can be strips of cloth, heavy rubber bands, neckties, handkerchiefs, or anything that can be knotted and twisted, preferably with a stick or pencil. Tighten the tourniquets, but check to be sure you can still feel a pulse in the patient’s wrists and feet.
Send for help.
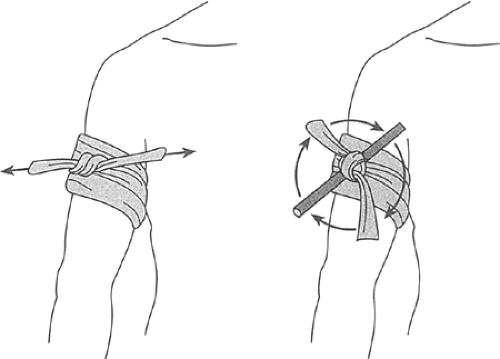 FIGURE 22-1 Treatment of left heart failure. The patient cannot breathe because the lungs are engorged with blood. Apply tourniquets as high as possible on the arms and legs. Twist the tourniquets tight until you can just feel a pulse in the wrists and feet. In 10 or 15 minutes, when the patient has begun to breathe easily, release one tourniquet. In another 15 minutes, retighten this tourniquet and loosen another. Continue rotating the tourniquets. |
In about 5 or 10 minutes, the victim will begin to breathe more easily. When this happens, loosen one of the tourniquets, leaving the other three tight. Every 15 minutes, retighten the slack tourniquet and loosen another one—in other words, rotate the tourniquets (Figure 22-1).
If necessary, you can keep up this rotation of tourniquets for several hours while you wait for help to arrive. If you are really in the wilderness, days from help, you can start to release the tourniquets one at a time after a couple of hours if the patient’s breathing seems easier. The tourniquets can always be reapplied, if needed.
Don’t try to make the patient walk about. Don’t throw cold water on his face. Don’t try to give him artificial respiration. Don’t try to make him eat or drink anything—he won’t want to, and he shouldn’t.
Coronary Heart Attacks
These will be either angina pectoris, myocardial ischemia, or a myocardial infarct. The symptom will be pain or some other acute discomfort, usually in the front half of the upper body. The pain may be over the heart or anywhere on the front of the chest. It may go up the sides of the neck toward the jaws. It often goes down the arms, particularly the left arm. Sometimes the pain will be in the very upper part of the abdomen, just at the lower end of the breastbone. The victim may think that he has acute indigestion, and he will almost always be frightened or apprehensive.
Angina Pectoris
If the patient is a known sufferer from angina pectoris, help him to take his nitroglycerin or another quick-acting coronary dilator. Help him find a place to rest, and watch him while the pain goes away. If it is a typical attack, and he is used to them, he will be able to resume activity when the pain has disappeared.
Myocardial Ischemia and Myocardial Infarction
The pain will not go away, even with rest or with nitroglycerin. The discomfort persists, and the patient is usually very apprehensive. You can do these things:
Put the patient at rest in a chair, couch, or bed. Sometimes he will want to move about and walk around in a frightened, agitated manner. Don’t let him do it. Make him be quiet.
Relieve the pain. Aspirin, whiskey, or any of the common pain-relieving agents available are all useful. Alcohol is good because it relieves pain and calms the frightened, agitated patient.
Send for help. Even if this means waiting for horses, helicopters, or some other means of travel out of rugged country, don’t move the patient until help arrives.
Don’t move the patient about or let him move himself about; keep him quiet. Don’t force him to eat; foods and liquids should be given in very small quantities as he desires them. Don’t apply artificial respiration or give stimulants such as caffeine.
“Stoppage” of the Heart
Acute left heart failure or coronary disease of any kind may cause the heart to stop pumping blood. This may happen in one of two ways: the ventricles may simply stop beating and hang motionless (ventricular standstill; see Chap. 12) or the ventricles may go into a feeble twitching motion, which cannot pump any blood (ventricular fibrillation; see Chap. 12).
In either case, the patient will fall as though shot. He will be motionless and he will not breathe. He is not yet dead, and he does not really have to die in many cases. Surprisingly often his life can be saved if there is someone nearby who knows what to do.
Note: Remember, the patient is not breathing and his heart is not beating. In 3 or 4 minutes the cells of the brain will begin to die for lack of oxygen. Whatever is to be done must be done at once.
To treat stoppage of the heart, you must first decide that it has happened. Making a diagnosis is the first step. The diagnosis of heart stoppage rests on two simple observations:
The patient is not breathing.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


