Gender is an important determinant of cardiovascular risk, and men generally develop cardiovascular disease earlier than women. Increased levels of high-sensitivity cardiac troponin I (hs-TnI) have been shown to be predictive of cardiovascular death, with stronger effects in women. However, it remains unclear whether the stronger association between hs-TnI and cardiovascular death in women is based on the ability of hs-TnI to predict myocardial infarction (MI) or heart failure (HF). Accordingly, we aimed to assess the influence of gender on the association between levels of hs-TnI and incident MI and HF. hs-TnI was measured in 5,060 women and 4,054 men participating in the prospective observational Nord-Trøndelag Health Study using the Architect STAT High-Sensitive Troponin assay. All subjects were free from known coronary heart disease at baseline. After a median follow-up of 5,105 and 6,169 days, 292 MIs and 209 admissions for HF were registered, respectively. In our total cohort, hs-TnI was associated with the incidence of both end points, with adjusted hazard ratio per 1 SD in log hs-TnI 1.19 (95% CI 1.02 to 1.39) for MI and 1.58 (1.38 to 1.82) for HF. The corresponding values for women and men were 1.35 (1.02 to 1.78) versus 1.13 (0.93 to 1.38) for MI and 1.55 (1.26 to 1.91) versus 1.61 (1.36 to 1.90) for HF. The C-index for hs-TnI was stronger for women than men for MI (p <0.001), and no such difference was observed for HF (p = 0.06). In conclusion, in the general population, the association between hs-TnI concentrations and MI is stronger in women than in men. For HF, the impact of gender on the prognostic value of hs-TnI is less pronounced. Increased levels of troponin I in women may thus reflect an adverse phenotype more prone to the development of cardiovascular disease.
Gender is an important determinant of cardiovascular risk, and men generally develop cardiovascular disease (CVD) earlier than women. Other risk factors, such as hypertension and smoking, also show gender-specific properties. Cardiac troponin T and troponin I (TnI) are both sensitive and specific indicators of myocardial injury most commonly used in the diagnosis of acute coronary syndromes. The use of high-sensitivity (hs−) assays enables quantitation of minute levels of circulating troponin in the general population. Furthermore, levels of both hs-troponin T and hs-TnI have been shown to be strongly associated with incident heart failure (HF) and cardiovascular death and to a lesser extent atherosclerotic events. More recent studies show a profound gender difference in the prognostic ability of hs-TnI on cardiovascular death, with an apparent stronger effect in women. However, it remains unclear whether the stronger association between hs-TnI and cardiovascular death in women is based on the ability of hs-TnI to predict myocardial infarction (MI) or HF. To further elucidate this effect of gender, we investigated the association between hs-TnI and incident MI and HF in women and men.
Methods
The Nord-Trøndelag Health Study (HUNT) is the largest population-based cohort in Norway, with >120,000 participants from the Nord-Trøndelag county. The following data originate from a subgroup of 9,712 participants from HUNT 2 (collected 1995 to 1997). The study was approved by the Regional Ethics Committee, and all participants provided informed consent. Subjects with known coronary heart disease (CHD) at baseline were excluded, leaving a total of 9,114 participants available for analyses.
Nonfasting venous blood samples were collected on study visit, centrifuged at room temperature, and frozen at −80°C. Samples used in this study underwent a thaw-freeze cycle in 2008 and were later stored at −20°C. For hs-TnI analyses, samples were shipped on dry ice to Akershus University Hospital, Lørenskog, Norway. hs-TnI was measured using an assay from Abbott Diagnostics: ARCHITECT STAT High Sensitive Troponin, details regarding analyses have recently been published elsewhere. The Modification of Diet in Renal Disease equation was used to assess estimated glomerular filtration rate (eGFR).
Data on admission for MI ( International Statistical Classification of Diseases, Ninth Revision or Tenth Revision , codes 410 or I21-I22) and HF (codes 428 or I50) were obtained from hospital records through December 31, 2010, and December 31, 2013, respectively. Only hospitalizations where these diagnoses were listed as the primary diagnosis were included. Data were obtained by linking the HUNT database to hospital databases in the county of Nord-Trøndelag, as described previously. Mortality status was also obtained for all participants as previously reported.
Data are given as either median (interquartile range) or absolute numbers (proportion). Continuous variables were analyzed using the Mann-Whitney U test and the Kruskal-Wallis test, and categorical variables with the Pearson chi-square test and the Fisher’s exact test, where appropriate. Levels of hs-TnI were transformed (ln) because of non-normal distribution. To determine diagnostic accuracy of hs-TnI on outcome, univariate C-indexes for hs-TnI were estimated using receiver-operating characteristics analysis. Cox proportional hazards regression models were generated to test the relation between hs-TnI and time to events. Participants were censored at the time of death or, for survivors, on January 1, 2011, for MI and January 1, 2014, for HF. In addition to MI and HF separately, a composite end point of cardiovascular death, MI, and HF, was constructed. For the composite end point, events were registered through December 31, 2010. Participants without events were censored at time of noncardiovascular death or, for survivors, on January 1, 2011. The multivariate Cox models were incrementally adjusted for gender (in entire cohort only), age, total and high-density lipoprotein cholesterol, history of hypertension, smoking status, history of diabetes, eGFR, and C-reactive protein. To examine a possible interaction between gender and levels of hs-TnI, interaction terms were created and entered in unadjusted and adjusted Cox proportional hazards models. Statistical significance was assumed at p <0.05. The analyses were performed using SPSS 22.0 (SPSS, Chicago, Illinois), STATA 14 (StataCorp LP, College Station, Texas), and MedCalc for Windows, version 16.2.0 (MedCalc Software, Ostend, Belgium).
Results
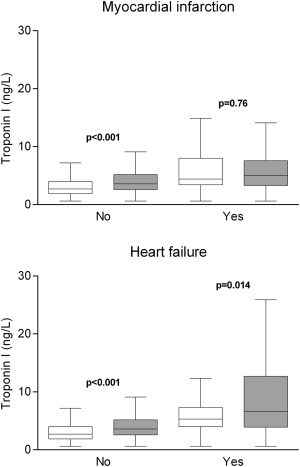
hs-TnI was measured in 5,060 women and 4,054 men, see Table 1 for baseline characteristics according to gender; 96.3% of the study subjects had hs-TnI levels at or above limit of detection (1.2 ng/L), 94.6% for women and 98.5% for men. Men displayed higher levels of hs-TnI than women (3.7 [2.6 to 5.3] vs 2.8 ng/L [1.9 to 4.0]; p <0.001). This difference was not evident in subjects with MI during follow-up (5.0 [3.3 to 7.6] vs 4.4 ng/L [3.4 to 8.0]; p = 0.76). Subjects with incident HF exhibited a gender disparity in hs-TnI levels similar to the entire cohort (6.6 [3.9 to 12.7] vs 5.3 ng/L [4.0 to 7.3]; p = 0.014; Figure 1 ). For all study end points, there was an increasing event rate with increasing gender-specific quartiles of hs-TnI ( Table 2 ).
| Variable | Women | Men | p | ||
|---|---|---|---|---|---|
| n | Value | n | Value | ||
| Age (years) | 5060 | 47.9 (35.9-62.0) | 4054 | 46.7 (35.7-59.3) | 0.002 |
| Current smokers | 4999 | 1493 (29.9%) | 4021 | 1121 (27.9%) | 0.040 |
| Weight (kg) | 5028 | 68.5 (62.0-77.0) | 4047 | 82.5 (75.0-90.5) | <0.001 |
| Body mass index (kg/m 2 ) | 5028 | 25.5 (23.0-28.6) | 4047 | 26.0 (24.1-28.3) | <0.001 |
| Waist hip ratio | 4965 | 0.79 (0.75-0.83) | 4045 | 0.90 (0.86-0.94) | <0.001 |
| Systolic blood pressure (mm Hg) | 5041 | 129 (117-147) | 4036 | 135 (125-148) | <0.001 |
| Diastolic blood pressure (mm Hg) | 5041 | 78 (71-86) | 4036 | 81 (74-89) | <0.001 |
| History of hypertension | 5037 | 1911 (37.9%) | 4035 | 1802 (44.7%) | <0.001 |
| History of diabetes mellitus | 5037 | 105 (2.1%) | 4053 | 106 (2.6%) | 0.093 |
| Glucose nonfasting (mmol/L) | 5060 | 5.1 (4.7-5.7) | 4054 | 5.2 (4.8-5.8) | <0.001 |
| Triglycerides nonfasting (mmol/L) | 5060 | 1.27 (0.91-1.84) | 4054 | 1.62 (1.13-2.31) | <0.001 |
| Total cholesterol (mmol/L) | 5060 | 5.8 (4.9-6.8) | 4054 | 5.7 (5.0-6.5) | <0.001 |
| HDL cholesterol (mmol/L) | 5060 | 1.5 (1.3-1.8) | 4051 | 1.2 (1.0-1.4) | <0.001 |
| Total/HDL cholesterol | 5060 | 3.8 (3.1-4.8) | 4051 | 4.6 (3.7-5.7) | <0.001 |
| eGFR (ml/min/1.73 m 2 ) | 5060 | 68.0 (60.5-75.7) | 4054 | 76.9 (69.3-85.0) | <0.001 |
| CRP (mg/L) | 5054 | 1.1 (0.4-2.7) | 4052 | 0.9 (0.4-2.1) | <0.001 |
| Troponin I (ng/L) | 5060 | 2.8 (1.9-4.0) | 4054 | 3.7 (2.6-5.3) | <0.001 |
| Gender specific quartiles of high-sensitivity troponin I | p | |||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | |||
| Myocardial infarction | Women | 4/1110 (0.4%) | 13/1408 (0.9%) | 23/1217 (1.9%) | 68/1325 (5.1%) | <0.001 |
| Men | 23/946 (2.4%) | 31/1073 (2.9%) | 44/1001 (4.4%) | 86/1034 (8.3%) | <0.001 | |
| p <0.001 | p <0.001 | p = 0.001 | p = 0.002 | |||
| Heart failure | Women | 2/1110 (0.2%) | 8/1408 (0.6%) | 17/1217 (1.4%) | 82/1325 (6.2%) | <0.001 |
| Men | 6/946 (0.6%) | 10/1073 (0.9%) | 22/1001 (2.2%) | 62/1034 (6.0%) | <0.001 | |
| p = 0.15 | p = 0.34 | p = 0.19 | p = 0.86 | |||
| Composite endpoint ∗ | Women | 12/1110 (1.1%) | 32/1408 (2.3%) | 60/1217 (4.9%) | 257/1325 (19.4%) | <0.001 |
| Men | 50/946 (5.3%) | 59/1073 (5.5%) | 77/1001 (7.7%) | 227/1034 (22.0%) | <0.001 | |
| p <0.001 | p <0.001 | p = 0.008 | p = 0.14 | |||
∗ Cardiovascular death, myocardial infarction or heart failure.
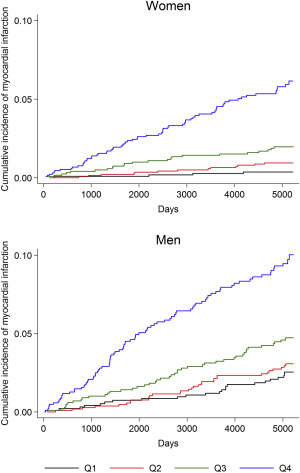
During a median follow-up of 5,105 days, there were 292 first hospitalizations for MI (108 women). There was a significant association between increasing levels of hs-TnI and hospitalization for MI ( Table 3 ). The association remained significant (hazard ratio [HR] per 1 SD in log hs-TnI 1.22 [95% CI 1.04 to 1.43]) after adjustment for gender, age, total and high-density lipoprotein cholesterol, history of hypertension, and smoking status (model #3). Further adjustment for history of diabetes, eGFR, and C-reactive protein (model #4) only marginally weakened this association (HR 1.19 [1.02 to 1.39]). In separate gender-specific models, the unadjusted HR associated with a 1 SD increase in the log of hs-TnI was 2.50 (2.13 to .94) in women and 1.63 (1.43 to 1.88) in men. In the fully adjusted model #4, the HRs in women and men were 1.35 (1.02 to 1.78) and 1.13 (0.93 to 1.38), respectively. The interaction with gender was statistically significant in both unadjusted (p <0.001) and adjusted (p = 0.023) models. Cumulative incidence plots by gender-specific quartiles of hs-TnI are shown in Figure 2 . The C-index for hs-TnI was 0.752 (0.708 to 0.797) in women and 0.644 (0.603 to 0.685) in men (p <0.001).
| Hazard ratio per 1 standard deviation in log hs-TnI (95% confidence interval) | ||||
|---|---|---|---|---|
| Model#1 ∗ | Model#2 | Model#3 | Model#4 | |
| Myocardial infarction | ||||
| Women | 2.50 (2.13-2.94) | 1.50 (1.15-1.96) | 1.43 (1.08-1.90) | 1.35 (1.02-1.78) |
| Men | 1.63 (1.43-1.88) | 1.12 (0.92-1.35) | 1.14 (0.94-1.39) | 1.13 (0.93-1.38) |
| Entire cohort | 1.96 (1.78-2.15) | 1.23 (1.05-1.43) | 1.22 (1.04-1.43) | 1.19 (1.02-1.39) |
| Heart failure | ||||
| Women | 2.65 (2.28-3.08) | 1.69 (1.32-2.16) | 1.59 (1.22-2.08) | 1.56 (1.20-2.04) |
| Men | 2.17 (1.93-2.44) | 1.80 (1.54-2.10) | 1.77 (1.51-2.08) | 1.61 (1.36-1.90) |
| Entire cohort | 2.27 (2.08-2.48) | 1.77 (1.55-2.02) | 1.72 (1.50-1.97) | 1.58 (1.38-1.82) |
| Composite endpoint † | ||||
| Women | 2.73 (2.52-2.96) | 1.63 (1.42-1.87) | 1.56 (1.35-1.80) | 1.50 (1.30-1.73) |
| Men | 1.85 (1.72-2.00) | 1.30 (1.16-1.45) | 1.31 (1.17-1.46) | 1.27 (1.14-1.42) |
| Entire cohort | 2.14 (2.03-2.25) | 1.41 (1.30-1.54) | 1.38 (1.27-1.51) | 1.34 (1.23-1.46) |
∗ Model #1, unadjusted; model #2, adjusted for gender (in entire cohort only) and age; model #3, adjusted for model #2 and total and HDL cholesterol, history of hypertension and smoking status; model #4, adjusted for model #3, history of diabetes, eGFR and CRP.
† Cardiovascular death, myocardial infarction or heart failure.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


