Foramen of Morgagni Hernia
Alberto de Hoyos
Giovanni Battista Morgagni,11 an Italian anatomist and pathologist, first described the rare anterior retrosternal diaphragmatic defect that now bears his name. He noted this condition while performing a postmortem examination on a person who died of a gangrenous colon herniated through the opening beneath the sternocostal junction. Because Larrey, Napoleon’s surgeon, described a surgical approach to the pericardial sac through an anterior retrosternal diaphragmatic defect, this area has also been termed the space of Larrey.
Anatomy
The embryology of the diaphragm is discussed in Chapter 51. Failure of formation or fusion of one or more of the four diaphragmatic components can result in a variety of diaphragmatic anomalies. Lack of fusion or muscularization of the pleuroperitoneal membrane anteriorly leads to a defect in the costosternal trigones known as the foramen of Morgagni. This triangular space is located between the muscle fibers of the xiphisternum and the costal margin fibers that insert on the central tendon (Fig. 54-1). A hernia of Morgagni is located just posterolateral to the sternum at the level of the seventh rib on either side of the xiphoid and has also been called retrosternal, parasternal, substernal, and subcostosternal. A hernia through the right sternocostal hiatus is referred to as a Morgagni hernia, whereas a hernia through the left hiatus is called a Larrey hernia. The internal mammary artery traverses this space to enter the rectus sheath and becomes the superior epigastric artery. The ligamentum teres defines the medial border of the hernia on either side. Because the peritoneum is intact, there is usually a true hernial sac. In most cases the hernia contains only omentum, but the transverse colon is occasionally involved and the small bowel, stomach, or liver only rarely. A left-sided defect is less likely to result in herniation because it is protected by the pericardium. Bilateral hernias have been described.
Incidence
Clinically evident hernias through the foramen of Morgagni are uncommon at any age. Despite their congenital etiology, they are detected less often in children than in adults. Comer and Clagett2 reported 50 patients (7%) with foramen of Morgagni hernia in a total of 750 patients with diaphragmatic hernias of all kinds over a 32-year period. Harrington5 listed only 7 foramen of Morgagni hernias (1.5%) in a series of 430 patients who were operated on for diaphragmatic hernia. Overall, the incidence of Morgagni hernia among all diaphragmatic defects in adults and children is 3% to 4%; it is the rarest of all diaphragmatic hernias. Foramen of Morgagni hernias may be associated with congenital abnormalities such as Down syndrome, pentalogy of Cantrell, Noonan syndrome, Prader–Willi syndrome, and Turner’s syndrome. In a review, Loong and Kocher10 found 47 case reports of children and 93 case reports of adults. About 90% of the hernias occur on the right, 8% are bilateral, and only 2% are limited to the left. Foramen of Morgagni hernias are detected more often in women than in men and more often in obese people than in those of average or below average weight.
Symptoms
In a literature review of 132 adult and pediatric cases, Berardi and associates1 reported that one third of patients are asymptomatic. Those with symptoms most frequently describe chronic gastrointestinal complaints such as pain or constipation from partial intermittent colonic obstruction. Symptoms due to intermittent gastric volvulus or small bowel obstruction are less frequent. Patients often complain only of vague epigastric or substernal fullness or a dull right subcostal discomfort. Diagnosis in these cases can be difficult and a missed diagnosis can lead to life-threatening complications.
Complete obstruction, incarceration, or strangulation with necrosis of a hollow viscus contained in a foramen of Morgagni hernia is rare and is associated with an acute or subacute presentation. In the series by Berardi,1 12 patients had complete bowel obstruction and 1 had gangrenous intestine. In the series of Loong and Kocher,10 14 of 47 children (14%) and 12 of 93 adults (12%) presented acutely. Forty percent of children presented subacutely.
Cardiorespiratory symptoms, mainly dyspnea and palpitations, are less common overall than gastrointestinal complaints. Although children are more often asymptomatic than adolescents and adults, they have about an equal incidence of respiratory and gastrointestinal symptoms.
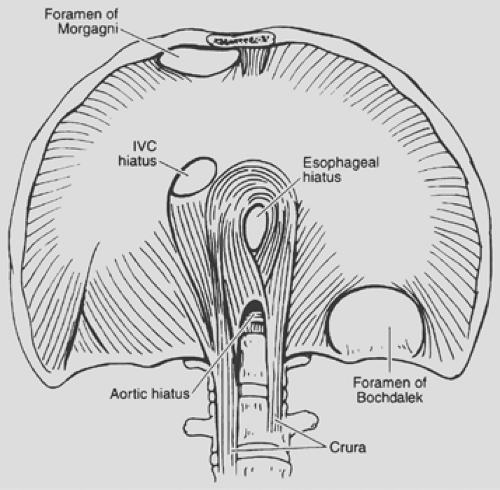 Figure 54-1. Illustration of posterolateral Bochdalek and anterior Morgagni diaphragmatic hernia. Note location of the latter between muscle fibers from the xiphisternum and from the costal arch that insert on the central tendon. (From Naunheim KS. Adult presentation of unusual diaphragmatic hernias. Chest Surg Clin North Am 1998;359;8359. With permission.) |
As with other hernias, conditions that produce prolonged or sudden severe increased intra-abdominal pressure can precipitate the onset of or exacerbate existing symptoms due to a foramen of Morgagni hernia. Velases and Sills13 reported that exercise and athletic activity may cause symptoms. Other precipitating events include trauma and pregnancy, as described by Ellyson and Parks3.
Diagnosis
The diagnosis of a foramen of Morgagni hernia is made by radi- ography, either prompted by symptoms or performed for unrelated reasons. In very small hernias, Lanuza9 described “the sign of the cane”: a curvilinear accumulation of fat continuous with the properitoneal fat line of the anterior abdominal wall. This sign suggests that a small anterior cardiophrenic mass may be a foramen of Morgagni hernia. More commonly, the standard chest radiograph shows obvious right, left, or bilateral pericardiophrenic abnormalities that are solid or contain air, depending on the contents of the hernia. The usual finding is a rounded opacity at the right cardiophrenic angle. The lateral chest film localizes this density to the anterior retrosternal space (Fig. 54-2). The opacification is generally due to omentum rising through the hernia defect. When the transverse colon, small bowel, or stomach herniates through the defect, an air–fluid level may be seen on chest films (Fig. 54-3). In adults, pericardial cyst, prominent fat pad, localized pneumothorax, bronchial carcinoma, atelectasis, and pneumonia in the cardiophrenic region, and atypical mediastinal tumor may mimic the radiographic features of herniation through the foramen of Morgagni. Diagnosis can be difficult and a missed diagnosis can lead to life-threatening complications such as obstruction and strangulation, as described by Harrington.6
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


