This chapter will highlight equipment essential to any percutaneous coronary intervention (PCI) procedure: coronary guide catheters, balloon catheters, and coronary guide wires. Details of coronary stent design and use are discussed in Chapter 14 (Stents). Specialized equipment for vascular access and closure, rotational atherectomy, laser atherectomy, cutting balloons, and structural heart disease are also addressed separately.
The initial decisions regarding the selection of guide catheters and guide wires and the need for other ancillary equipment are critical. Often the difference between an apparently effortless coronary intervention and one that appears laborious or challenging revolves around obtaining adequate guide support and guide-wire mobility.
PCI equipment consists of three basic elements: the guiding catheter, the balloon-stent catheter, and the coronary guide wire. Typically, the choice of equipment remains the same regardless of whether the procedure is performed from the femoral or radial approach, although adequate support may be more difficult to obtain from the radial approach. This chapter focuses on PCI from the femoral approach, as femoral artery access has historically been the mainstay in performing coronary interventions.
GUIDING CATHETERS
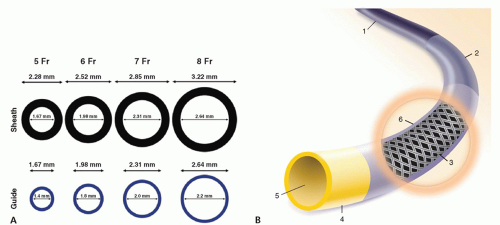
Guide catheters are dedicated large-bore catheters used to deliver coronary guide wires and balloon catheters to the target vessel. Sizes of catheters are shown in Figure 13-1A. The traditional guide catheter was constructed with three layers: an outer nylon layer, a middle braided wire mesh layer, and an inner hydrophilic coated layer (Fig. 13-1B). Compared with simple diagnostic catheters, the braided guide catheter has thinner walls and a larger internal diameter (ID) through which balloon and stent delivery catheters can be inserted. Guide catheters are stiffer than diagnostic catheters, which enables them to provide support for balloon-stent catheters to traverse the coronary stenosis. Manipulation of guide catheters differs from that of diagnostic catheters. The tip of the guide catheter is larger and not tapered, making it more likely to obstruct the coronary ostium, causing pressure dampening upon engagement (1, 2, 3).
FIGURE 13-1 A: Sheath sizes and guide catheter inner and outer diameters. (From: From AM, et al. Catheter Cardiovasc Interv. 2010;76(7):911-916, with permission.) B: Layers of guide catheter. Illustration of a guiding catheter shows stiffer body (1); variable softer primary curve (2); wire braiding (3); atraumatic tip (4); large lumen (optional radioopaque marker) (5); lubrious coating (Boston Scientific, Inc.).
Guide catheter choice is dependent on many factors (Table 13-1) such as the patient’s body habitus; age; anatomy of the ascending aorta and aortic root; coronary artery anatomic variants, diseased native coronary arteries or bypass grafts; ostial, proximal, or distal location of the target lesions; bifurcation disease; degree of tortuosity; and calcification in the coronary artery. The French size, the shape, the need for side holes, and the length of the catheter are also important factors. Many manufacturers supply a wide variety of preshaped guide catheters with various sizes and features (Table 13-2).
Guide catheters can be used as either active or passive guides. Most guide catheters are designed to provide passive support, meaning that they are placed at the ostium of the vessel. They provide adequate support to facilitate the intervention through their stiffness, back support against the aortic wall, and shape. An active guide is one that is smaller (≤6 Fr) and more flexible and that can be deeply seated or advanced past the ostium down into the vessel to provide additional support. This technique is less commonly used as there is a risk of damage to the vessel and ischemia to the territory supplied. However, in difficult cases, active support may be required to pass equipment. The Guideliner device (described below) provides a form of active support (4).
TABLE 13-1 Factors to Consider in Choosing Guide Catheters
Complex procedure, CTO, calcified and tortuous vessel, requires extra support — choose 7 or 8 Fr
Shape of the guide (need for back wall support)
Aorta is dilated or enlarged, tortuous—choose longer length between primary and secondary curve for left guides
Length
PCI through long bypass grafts or the LIMA into the native arteries—choose 90-cm guide
Side holes
Small ostia, pressure will damp or ventricularize, need to deeply intubate guide—choose a guide with side holes
Aortic Configuration
RCA Guides
Normal
JR 3.5,4 AL 0.75, 1 Hockey Stick AR 1
Dilated
JR4.5, 4 AL 1.5,2, AR 2
Narrow
JR3, LIMA
Aortic Configuration
Left Coronary Guides
Normal
EBU/XB3.5-4, JL4, AL 1.5-2
Dilated
EBU/XB4or>, JL4.5or>, Voda
Narrow
EBU/XB 3-3.5, JL 3-3.5
Other Circumstances That Will Dictate Guide Selection
Coronary Anatomy and Orientation
Ostial disease
Use side holes, use guide that will be easy to disengage
Short Left Main/Dual Left Coronary Ostial
Need to subselect LAD or LCX
Sheperd’s Crook right
Need extra support, consider AL guide
Bypass Grafts Orientation
To right coronaries
Horizontal or inferior
To left coronaries
Horizontal or superior
TABLE 13-2 Guide Catheter Styles and Lengths
Standard Shapes (cm)
Right Judkins/Femoral—JR or FR (3.0, 3.5, 4.0, 4.5, 5.0, 6.0)
Left Judkins/Femoral—JL or FL (3.0, 3.5, 4.0, 4.5, 5.0, 6.0)
Right Amplatz—AR1, 2
Left Amplatz—AL 0.75, 1, 1.5, 2, 3
Multipurpose
Specialty Curves
Right bypass
Left bypass
Internal mammary
“Q” curve
Voda curve
“C” curve (3.0, 3.5, 4.0, 4.5, 5.0)
Hockey stick
Extra backup support—EBU or XB (3.0, 3.5, 3.75, 4.0)
Guide Catheter Sizes
Today, 6-Fr guiding catheters are the most commonly used catheters. Larger guiding catheters (7 Fr or 8 Fr) may be needed for kissing balloons/stents, rotablator burrs larger than 2 mm, and some cutting balloons (Table 13-3). Because the limitation of the device is its external diameter, it is important to know the ID of the guides you select. Many of the newer 6-Fr guide catheters have the braided wire mesh embedded into the nylon outer layer, increasing the ID significantly (up to 0.071”) (Fig. 13-1). As a result, the vast majority of interventions can now be performed with a 6-Fr guide.
From both the femoral and the radial approach, sheath and guide catheter diameter impacts the procedural outcomes and complications. The 6-Fr guide is preferred for routine procedures that do not require large devices. The 8-Fr guides are reserved for larger devices or lesions requiring two simultaneous over-the-wire (OTW) systems. In some labs, 7-Fr guides are used as a compromise. A variety of periprocedural complications (bleeding, dissection) are associated with the use of 7- or 8-Fr guides than with 6-Fr guides. Although patients receiving larger guides almost certainly have more complex lesions and comorbidities, mortality rates appear higher with larger guides (Fig. 13-2). Hence, the general adage is “bigger is not better” (4, 5).
Only gold members can continue reading. Log In or Register to continue