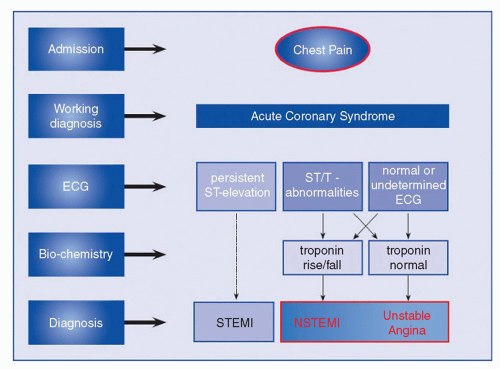
The acute coronary syndromes (ACS) include unstable angina (UA), non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI) (Fig. 16-1). Patients presenting with chest pain without persistent ST-elevation are typically admitted to the hospital with the diagnosis of non-ST-elevation ACS (NSTE-ACS), and later classified into UA or NSTEMI on the basis of cardiac biomarkers.
Patients with ACS constitute the vast majority of patients (>80%) who will require percutaneous coronary intervention (PCI). With the publication of the COURAGE trial and increasing scrutiny from payers, the use of PCI for stable angina is increasingly reserved for refractory symptoms(1).
EPIDEMIOLOGY
In the United States, there are 1.19 million hospital admissions for ACS annually. UA/NSTEMI patients constitute 845 million, or ∽71% of the total, while STEMI patients make up a smaller fraction. The overall incidence of both NSTE-ACS and STEMI has decreased in the past decade, likely due to decreased smoking rates and improved medical therapy (especially statins) (2).
The acute in-hospital mortality of STEMI (7%) is higher than that of NSTE-ACS (3%—5%), but equalizes by 6 months. Longerterm follow-up demonstrates that NSTE-ACS has a higher mortality rate than STEMI. This is explained by different patient profiles: NSTE-ACS patients on average tend to be older and have more comorbidities such as diabetes and renal failure, whereas STEMI patients tend to be younger smokers.
PATHOLOGY
ACS result from coronary artery obstruction causing myocardial ischemia and NSTEMI and STEMI myocardial necrosis. Acute coronary artery obstruction typically results from thrombosis of a ruptured coronary plaque, with or without concomitant vasoconstriction. In contrast to the previous conception that coronary artery disease (CAD) is a slowly progressive disease, the current understanding of CAD (see Chapter 1) is that of a stuttering inflammatory process of repeated plaque rupture and healing on top of a lipid core. Abrupt thrombotic occlusion may rapidly progress in plaques that are not obstructive at baseline.
Coronary thrombosis involves endothelial dysfunction and disruption, platelet activation, and circulating coagulation proteins. The platelet is a central actor and regulates the process of thrombosis (see Chapter 5). When endothelial cells are injured, thrombosis begins with rapid adhesion of platelets to the site of injury. Within seconds, the platelets are activated, degranulate, and recruit additional platelets to the developing thrombus. The secretory granules release adenosine diphosphate (ADP), which stimulates further platelet activation, and thrombin, which initiates the coagulation system. Thromboxane is generated from the platelet phospholipase A2, and has an additional effect on platelet activation. Ultimately, glycoprotein (GP) IIb/IIIa receptors on the platelet are activated. GP IIb/IIIa receptors bind to fibrinogen, cross-linking platelets together. Repetitive platelet activation and fibrinogen cross-linking brings about platelet aggregation, which can then lead to occlusive thrombus formation. Although there are multiple pathways to platelet activation, the platelet GP IIb/IIIa receptor is the final common pathway in platelet aggregation that would lead to NSTEMI.
FIGURE 16-1 Spectrum of ACS. (From: Hamm, et al. Eur Heart J. 2011;32(23):2999-3054, with permission.)
When plaque rupture results in complete (100%) thrombotic occlusion and is sustained, the myocardial infarction (MI) that results is typically transmural and associated with ST-segment elevation. Without reperfusion, this ultimately leads to a Q-wave infarction. With subtotal (99% or less) or transient occlusion, the presentation may be either UA or NSTEMI, depending upon the degree and duration of ischemia. When ischemia is sufficient to cause myonecrosis detectable by serum biomarkers, NSTEMI is diagnosed. With the use of sensitive troponin assays, patients who would have formerly been categorized as UA (based on negative creatine kinase) are increasingly diagnosed as NSTEMI.
Other less common causes of ACS include spontaneous coronary dissection, spasm (Prinzmetal angina, cocaine), inflammatory arteritis, trauma, and thromboembolism. These rare causes should be considered in patients lacking CAD risk factors. For instance, a younger peripartum woman with chest pain and changes in electrocardiogram (ECG) may be more likely to have spasm or coronary dissection than atherosclerotic disease.
CLINICAL PRESENTATION
The clinical presentation of ACS classically includes substernal chest discomfort associated with diaphoresis and dyspnea. This sensation may variably be described as pressure or sharp pain, depending on the patient. The chest discomfort may radiate to the left arm, and also to the shoulder, neck, or jaw. Relief of chest pain with nitroglycerin and exacerbation of the chest pain with manual pressure may point toward a noncardiac cause for chest pain, but these signs are insufficiently reliable for clinical diagnosis.
Atypical presentations occur frequently, particularly among diabetic patients and women. Dyspnea, epigastric pain, nausea, syncope, or unexplained tachycardia may be the only symptoms to suggest a cardiac pathology.
Physical examination of the ACS patients is often unremarkable. Signs of left ventricular dysfunction (rales, third heart sound, hypotension, jugular venous distention) or cardiogenic shock (cold clammy extremities, tachycardia) may be present in patients with extensive MI or prior injury. Transient ischemia may be associated with papillary muscle dysfunction and intermittent murmur of mitral regurgitation.
INITIAL DIAGNOSIS
Patients with chest pain require prompt triage and risk assessment in an emergency room. An ECG should be immediately performed, with a goal of within 10 minutes. Serial ECGs are also recommended for patients with nondiagnostic ECGs or for those who continue to be symptomatic. Comparison with prior ECGs can be extremely valuable, particularly in patients with baseline abnormalities such as hypertrophy or early repolarization. ECGs should be reviewed for ST-segment elevation (≥1 mm in two contiguous leads) or new left bundle branch block, which may indicate acute STEMI. Isolated ST-segment depression in right precordial leads (V1-V3) with tall R waves may indicate a true posterior infarction, which should also be treated as a STEMI. NSTE-ACS may present as ST-segment depression or T-wave inversions, or be electrically silent. Dynamic ST-segment or T-wave changes increase the specificity of the ECG for ACS.
Unfortunately, the history and physical examination, and ECG are sufficient to diagnose ACS in only <50% of cases. Cardiac biomarkers should thus be drawn on all patients with suspected ACS. Biomarkers may not be elevated in the first 4 hours after the onset of symptoms, and thus serial biomarkers should be drawn at 6- or 8-hour intervals. The preferred cardiac biomarker is the troponin assay (cTnI or cTnT), which has a very high (>95%) sensitivity for myocardial injury. Ultrahigh-sensitivity (>99%) troponin assays are increasingly becoming available, and may reduce the time to diagnosis of ACS (3). Abnormal troponin levels connote an increased risk for major adverse cardiac events and death, with higher concentrations indicating progressively elevated risk (4). The specificity of the cardiac troponin for ACS is reported to be very high (>95%) when used in patients with chest pain. However, when used in a patient population broader than that in clinical trials, the test may be positive for reasons besides ACS, and there may still be a role for less-sensitive (but more specific) markers such as CK-MB. For instance, following PCI, troponin assays are overly sensitive to clinically silent periprocedural necrosis, and do not carry the same prognostic value as elevations in CK-MB (5).
B-type natriuretic peptide (BNP) is increasingly used as a cardiac biomarker. Elevated levels may reflect either acquired or preexisting left ventricular dysfunction and are associated with an increased risk of complications (4).
IS IT ACS?
With the advent of high-sensitivity troponin assays as the preferred cardiac marker, one of the most common consultations received by the interventional cardiologist is for the positive troponin, which in the absence of chest pain is often caused by demand ischemia, heart failure, or renal failure, rather than ACS (6). The 2012 universal definition of MI (Table 16-1) includes patients with positive biomarkers with either ischemic symptoms, ECG changes of ischemia or infarction, or echocardiographic evidence of infarction. This definition includes infarctions because of ACS, supply-demand imbalance, sudden cardiac death, PCI complications, or post-CABG (7). The terminology is thus muddled, in that a patient may have a MI without having an ACS (NSTEMI or STEMI), particularly when nondiagnostic symptoms (especially dyspnea, hypotension) and ECG (T-wave inversions) are present. Changes in the concentration of troponin may be helpful in differentiating acute from chronic causes of myocardial damage, with a rise of 20% typically being used as a criterion for an acute injury, especially in patients with renal failure, heart failure, or left ventricular hypertrophy (8).
Antithrombotic therapies and PCI are beneficial only for patients with primary acute thrombotic coronary events. An incorrect diagnosis at best will be a distraction from underlying illness, at worst a therapeutic misadventure that will result in hemorrhagic or vascular complications.
INITIAL MEDICAL MANAGEMENT
ACC/AHA Guidelines for the management of UA/NSTEMI were issued in complete form in 2007 (9) and updated in 2011 (10). A thorough review of these guidelines is suggested for board preparation.
TABLE 16-1 Clinical Classification of Different Types of Myocardial Infarction
Type 1
Spontaneous myocardial infarction related to atherosclerotic plaque rupture, fissuring, erosion, or dissection with resulting intraluminal thrombus in one or more coronary arteries leading to decreased myocardial blood flow or distal platelet emboli with ensuing myocyte necrosis.
Type 2
Myocardial injury with necrosis where a condition other than CAD contributes to an imbalance between myocardial oxygen supply and/or demand, e.g. coronary endothelial dysfunction, coronary artery spasm, coronary embolism, tachy-/bradyarrhythmias, anemia, respiratory failure, hypotension, and hypertension with or without LVH.
Type 3
Cardiac death with symptoms suggestive of myocardial ischemia and presumed new ischemic ECG changes or new LBBB, but death occurring before blood samples could be obtained or before cardiac biomarkers could rise.
Type 4a
Myocardial infarction associated with PCI
Type 4b
Myocardial infarction associated with stent thrombosis
Type 5
Myocardial infarction associated with CABG
From: Thygesen Ket al. J Am Coll Cardiol. 2012; 60:1581-98, with permission.
Anti-Ischemic Therapies
Anti-ischemic therapies reduce myocardial oxygen demand or increase myocardial oxygen supply. Recommended anti-ischemic therapies are listed in Table 16-2. Nonpharmacologic therapies include bed rest and supplemental oxygen. Nitroglycerin can cause coronary vasodilatation and increase myocardial blood flow. β blockers and calcium-channel blockers reduce myocardial demand by reducing heart rate, contractility, and afterload. βblockers should not be administered for patients with shock, heart failure, or heart block. Morphine is reserved for angina refractory to nitroglycerin, but by relieving pain and anxiety, it also reduces myocardial oxygen demand.
Risk Stratification
Early risk stratification for ischemic complications is critical to form a management strategy for the heterogeneous NSTE-ACS population. A focused history and physical examination, a prompt electrocardiogram (ECG), and cardiac biomarkers, as described previously, will help distinguish UA and NSTEMI from noncardiac chest pain. Patients with a normal ECG and cardiac biomarkers can be safely sent for noninvasive stress testing for further risk assessment.
For those with UA/NSTEMI, risk-stratification models such as the TIMI or GRACE risk score should be used to further identify those patients at high risk for cardiovascular death, recurrent MI, or urgent revascularization (Fig. 16-2, Table 16-3). The TIMI risk score is simpler to remember, but has a less discriminating power. Patients at low risk for cardiac events (TIMI score < 3, GRACE score < 108) are candidates for a conservative approach, whereas patients with a moderate or high score are best treated with an invasive approach (see below) (11, 12).
TABLE 16-2 Recommended Anti-ischemic Therapies
Class I
1)
Bed rest with continuous ECG monitoring
2)
Supplemental oxygen in patients with respiratory distress or hypoxemia
3)
Nitroglycerin for ischemic symptoms, heart failure, or hypertension
4)
Oral β blockers for patients without shock, heart failure, or heart block
5)
ACE inhibitors or angiotensin-receptor blockers within 24 hours in patients with left ventricular dysfunction
Class IIa
6)
Morphine for chest discomfort refractory to nitroglycerin
7)
Intravenous β blockers for patients without contraindications
Only gold members can continue reading. Log In or Register to continue