Empyema
Presentation
A 60-year-old woman presents to the emergency department and is admitted to the hospital with elevated temperature. She has been experiencing fatigue and myalgia for the past several days, but on the day of admission, she develops shaking chills and pleuritic chest pain.
Her past medical history is significant for a recent dental extraction of an abscessed tooth, hypertension, and diabetes. She is a long-time smoker of 40 packyears. On physical examination, the patient appears toxic. Temperature is 104.3°F, pulse is 110 beats/min, and blood pressure is 100/60 mm Hg. She has no cervical adenopathy. Her extraction site appears to be healing, and there is no tenderness over this area. There are diminished breath sounds over the left hemithorax, and there is tenderness over her left chest.
Differential Diagnosis
The high temperature with chills this patient is experiencing is most likely of infectious etiology. Pneumonia, lung abscess, and empyema should be considered.
Case Continued
Blood cultures and laboratories are sent. The patient’s white blood cell (WBC) count is 16,000/mm3. Broad-spectrum antibiotics and intravenous fluids are immediately begun. Chest x-rays are performed.
▪ Chest X-rays
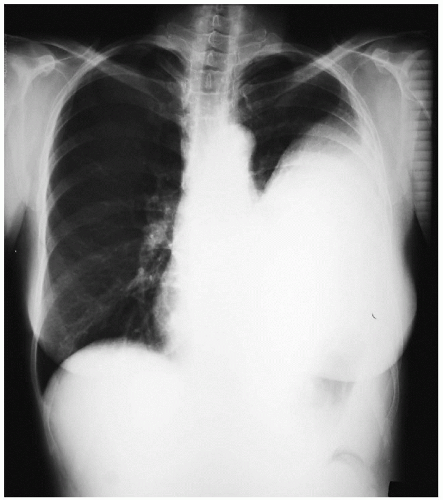 Figure 30-1 |
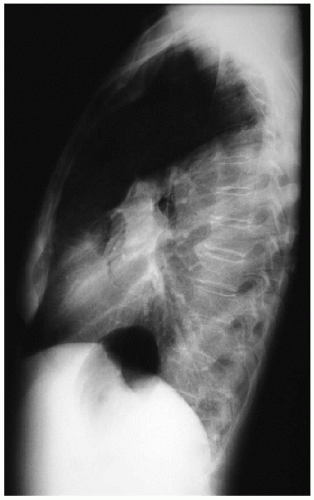 Figure 30-2 |
Chest X-ray Report
There is opacification of the lower two thirds of the left hemithorax. There are no masses or effusion in the left chest. The left heart border is not clearly defined. ▪
Case Continued
The patient had a chest tube placed into the collection on the left side at the bedside. More than 1,000 mL of foul-smelling, purulent material was removed. The Gram stain showed gram-positive rods, and the culture grew Actinomyces meyeri. The temperature returned to normal over the next 2 days.
Diagnosis
Empyema.



