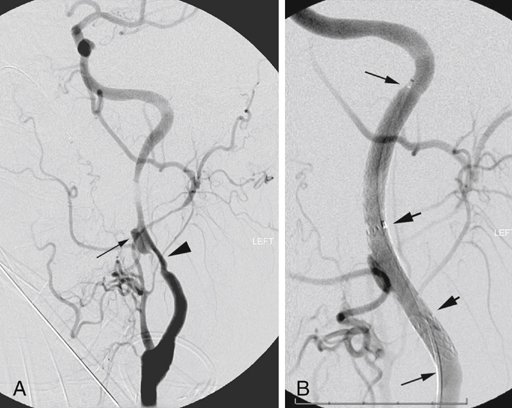
In the event of a propagated clot extending into the carotid siphon that is not removed using the previous maneuver, judicious use of a 2- to 3-Fr Fogarty embolectomy catheter may be attempted, but the catheter must not be advanced or inflated beyond even minimal resistance owing to the risk of a carotid–cavernous sinus fistula. We would favor using intraoperative fluoroscopic guidance for any mechanical attempts to remove distal thrombus. Endovascular rescue approaches can also be used to allow removal of downstream thrombus or correction of associated intimal or atheromatous occlusive downstream pathology (Figure 1). Such approaches have become much more available with the widespread availability of hybrid operating rooms.
Early Postoperative Recognition and Management of Acute Stroke After Carotid Endarterectomy
Surgical Reexploration
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine
