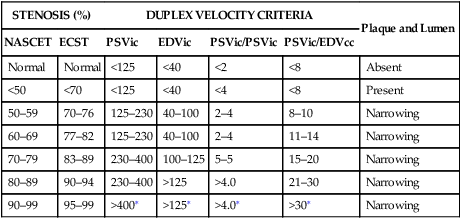
Guidelines recommend expressing the degree of ICA stenosis as a percentage of stenosis in relation to the distal normal ICA (NASCET [North American Symptomatic Carotid Endarterectomy Trial] stenosis) in routine clinical practice (see Chapter 6). Expressing the stenosis as a percentage of the bulb diameter (ECST [European Carotid Surgery Trial] stenosis) is needed in certain studies because it reflects the plaque volume and it is directly related to stroke risk. To avoid confusion, it should be remembered that the same velocities can be expressed in both NASCET and ECST grades of stenosis (Table 1). TABLE 1 Guidelines for Expressing Degree of Stenosis in the Internal Carotid Artery ∗In cases of trickle flow, these velocities might not be detectable (see text). The criteria for different velocity ratios were initially tailored to screening and selecting patients for subsequent angiography. Thus, they had a high sensitivity at the expense of specificity. The aim was to not miss a patient with a stenosis greater than 60% (NASCET). However, subsequently, with the need to make decisions to proceed to carotid endarterectomy without angiography, the criteria were tailored to have equally high sensitivity and specificity. The criteria listed in Table 1 are based on the latter option, with emphasis on obtaining the highest combined sensitivity and specificity for surgically important grades greater than 70% (ECST) as indicated by the ECST trial, 60% (NASCET) as indicated by the Asymptomatic Carotid Atherosclerosis Study (ACAS) trial, and 70% (NASCET) as indicated by the NASCET trial.
Duplex Scanning and Spectral Analysis of Carotid Bifurcation Atherosclerotic Disease
Important Concepts
STENOSIS (%)
DUPLEX VELOCITY CRITERIA
Plaque and Lumen
NASCET
ECST
PSVic
EDVic
PSVic/PSVic
PSVic/EDVcc
Normal
Normal
<125
<40
<2
<8
Absent
<50
<70
<125
<40
<4
<8
Present
50–59
70–76
125–230
40–100
2–4
8–10
Narrowing
60–69
77–82
125–230
40–100
2–4
11–14
Narrowing
70–79
83–89
230–400
100–125
5–5
15–20
Narrowing
80–89
90–94
230–400
>125
>4.0
21–30
Narrowing
90–99
95–99
>400∗
>125∗
>4.0∗
>30∗
Narrowing
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


