Type III hyperlipoproteinemia is a rare familial disease characterized by marked elevations of serum cholesterol and triglyceride levels caused by an accumulation of remnant lipoproteins in apolipoprotein E2/E2 homozygotes. It is associated with an increased risk for premature atherosclerotic vascular disease. A 55-year-old woman was diagnosed as having type III hyperlipoproteinemia on the basis of skin lesions, serum lipid levels, lipid electrophoresis, and apolipoprotein E genotyping and stable angina pectoris on the basis of typical symptoms and treadmill exercise electrocardiographic results. After 1 year of combination therapy with atorvastatin and fenofibrate, skin xanthomata disappeared, leaving minimal remnants. In addition, there was no exertional chest pain, and treadmill exercise electrocardiographic results were negative. This finding was confirmed by coronary computed tomographic angiography. This case suggests that proper medical therapy can induce the regression of uncomplicated coronary lesions in type III hyperlipoproteinemia.
Case Description
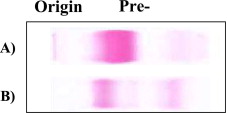
A 55-year-old woman visited the hospital because of progressive systemic skin lesions for 2 years and chest pain for 4 months. Anterior chest pain without radiation appeared during moderate exercise and was reduced with several minutes of rest. The patient’s body mass index was 25.4 kg/m 2 (height 160 cm, weight 65 kg). She exhibited extensive eruptive and tuberous xanthomata over the elbow and buttock areas and yellowish orange discoloration of the palmar creases ( Figure 1 ). Her mother and brother had experienced acute myocardial infarctions. Fasting cholesterol and triglyceride levels were 747 and 1,315 mg/dl, respectively. Lipid electrophoresis revealed a broad β-band pattern ( Figure 2 ), and polymerase chain reaction multiplex amplification refractory mutation system showed apolipoprotein E2/E2 (Arg 158 → Cys) genotype. Treadmill exercise electrocardiography showed 1.5-mm downsloping depression of the ST segment in leads II, III, aVF, and V 4 to V 6 , with T-wave inversion at 8.9 METs ( Figure 3 ), and the patient described chest pain. She refused any further invasive procedures and was managed with aspirin, nitrate, a calcium channel blocker, and a β blocker. In addition, fenofibrate 160 mg and atorvastatin 10 mg were administered.
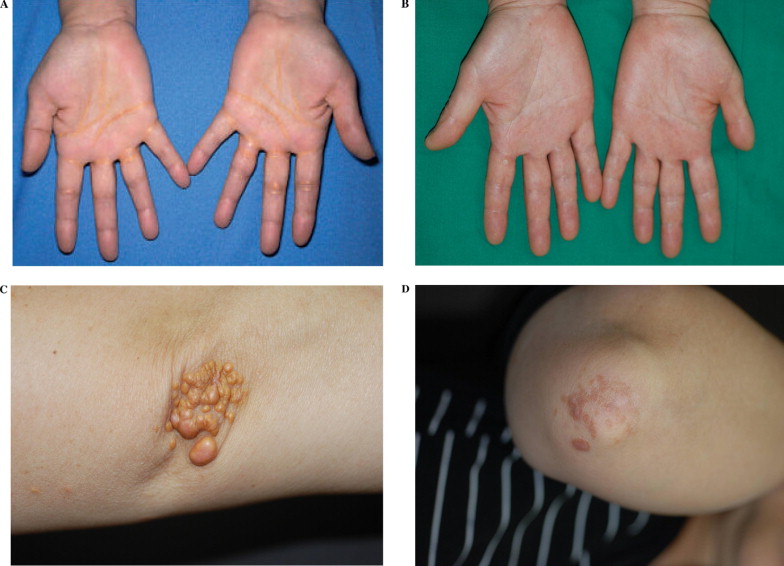
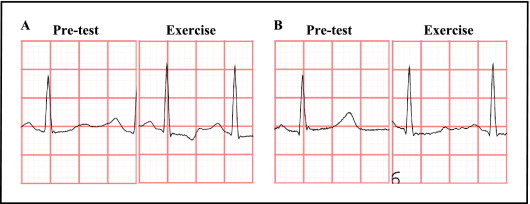
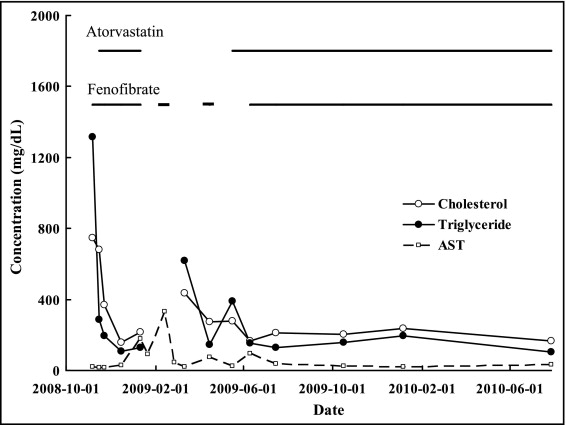
After 1 month of medications and diet control, fasting cholesterol and triglyceride levels decreased to 157 mg/dl and 108 mg/dl, respectively ( Figure 4 ). During follow-up, aspartate aminotransferase and alanine aminotransferase levels increased to 178 and 232 IU/L, respectively, and lipid-lowering drugs were discontinued. For 3 months, repeated administrations of fenofibrate increased aspartate aminotransferase and alanine aminotransferase levels. Hence afterward, atorvastatin was initially administered and fenofibrate was added again later. After that, fasting cholesterol (164 to 237 mg/dl) and triglyceride (105 to 193 mg/dl) levels were well controlled. After 3 months of repeat administration of lipid-lowering drugs, the hard consistency of the xanthomata was softened. After 1 year, the skin lesions disappeared, leaving minimal remnants ( Figure 1 ). Treadmill exercise electrocardiographic results were negative ( Figure 3 ). On coronary computed tomographic angiography, no stenotic lesions of the coronary arteries were observed ( Figure 5 ). After the discontinuation of antianginal drugs, she did not experience exertional chest pain.