Hypertension and left ventricular (LV) hypertrophy are both more common in blacks than in whites. The aim of the present study was to test the hypothesis that blood pressure (BP) has a differential effect on the LV geometry types in black versus white asymptomatic young adults. As a part of the Bogalusa Heart Study, echocardiography and cardiovascular risk factor measurements were performed in 780 white and 343 black subjects (aged 24 to 47 years). Four LV geometry types were identified as normal, concentric remodeling, eccentric, and concentric hypertrophy. Compared to the white subjects, the black subjects had a greater prevalence of eccentric (15.7% vs 9.1%, p <0.001) and concentric (9.3% vs 4.1%, p <0.001) hypertrophy. On multivariate logistic regression analyses, adjusting for age, gender, body mass index, lipids, and glucose, the black subjects showed a significantly stronger association of LV concentric hypertrophy with BP (systolic BP, odds ratio [OR] 3.74, p <0.001; diastolic BP, OR 2.86, p <0.001) than whites (systolic BP, OR 1.50, p = 0.037; and diastolic BP, OR 1.35, p = 0.167), with p values for the race difference of 0.007 for systolic BP and 0.026 for diastolic BP. LV eccentric hypertrophy showed similar trends for the race difference in the ORs; however, the association between eccentric hypertrophy and BP was not significant in the white subjects. With respect to LV concentric remodeling, its association with BP was not significant in either blacks or whites. In conclusion, elevated BP levels have a greater detrimental effect on LV hypertrophy patterns in the black versus white young adults. These findings suggest that blacks might be more susceptible than whites to BP-related adverse cardiac remodeling.
Hypertension is an important risk factor for left ventricular (LV) hypertrophy, a subclinical cardiovascular disease that represents one of the strongest independent predictors of cardiovascular morbidity and mortality in the general population. Although it is well known that hypertension and LV hypertrophy are both more common in blacks than in their white counterparts, data on whether high blood pressure (BP) levels are more closely associated with an increased LV mass in blacks than in whites have not been consistent. Also, information has been limited on how BP levels influence LV geometry and remodeling in black and white young adults. The objective of the present study was to examine the racial differences in the effect of BP on LV geometric patterns in black and white young adults enrolled in the Bogalusa Heart Study.
Methods
As a part of the Bogalusa Heart Study, a biracial (black–white) community-based investigation of the early nature history of cardiovascular disease, a total of 1,123 subjects (780 whites and 343 blacks, 42.2% men, age 24 to 47 years), who were residing in the community of Bogalusa, Louisiana, were examined for LV dimensions and cardiovascular risk factor variables in 2004 to 2008. All subjects in the present study gave informed consent for examination. The institutional review board of the Tulane University Medical Center approved the study protocols.
The BP levels were measured from the right arm of the subjects, with the subjects in a sitting position by 2 trained observers (3 replicates each). The systolic BP (SBP) and diastolic BP (DBP) were recorded at the first and fifth Korotkoff phases, respectively, using a mercury sphygmomanometer. The average of the 6 BP readings was used for analysis. For the 147 subjects who were taking medications for hypertension at the examination, the recorded BP values were adjusted by adding 10 mm Hg to the SBP and 5 mm Hg to the DBP, as determined by the average treatment effects. We tried to include these subjects because they represented a subgroup with the greatest BP.
The LV dimensions were assessed using 2-dimensional guided M-mode echocardiography, with 2.25- and 3.5-MHz transducers according to the American Society of Echocardiography recommendations. The parasternal long- and short-axis views were used to measure the LV end-diastolic and end-systolic measurements in duplicate, which were then averaged. The LV mass was calculated from a necropsy-validated formula according to thick wall prolate ellipsoidal geometry. To take the body size into account, the LV mass was indexed for body height (m 2.7 ). The LV relative wall thickness was calculated as the septal wall thickness plus the posterior wall thickness divided by the LV end-diastolic diameter. The presence of LV hypertrophy was defined by a gender-specific cutoff of the LV mass index of >46.7g/m 2.7 for women and >49.2g/m 2.7 for men. The LV geometry was considered concentric when the relative wall thickness was >0.42. Four different patterns of LV geometry were defined: normal LV geometry, normal relative wall thickness with no LV hypertrophy; concentric remodeling, increased relative wall thickness but no LV hypertrophy; eccentric hypertrophy, normal relative wall thickness with LV hypertrophy; and concentric hypertrophy, increased relative wall thickness with LV hypertrophy.
The cholesterol and triglyceride serum levels were assayed using enzymatic procedures on a Hitachi 902 automatic analyzer (Roche Diagnostics, Indianapolis, Indiana). The glucose levels were measured as a part of a multiple chemistry profile (SMA20) using enzymatic procedures with a multichannel Olympus, Au-5000 analyzer (Olympus, Lake Success, New York). The laboratory was monitored for precision and accuracy of lipid measurements by the Lipid Standardization and Surveillance Program of the Centers for Disease Control and Prevention (Atlanta, Georgia).
All the statistical analyses were performed using SAS, version 9.1 (SAS Institute, Cary, North Carolina). Analyses of covariance were performed using general linear models to test the differences in the study variables between the normal group and LV geometric remodeling groups. Multivariate logistic regression analyses were performed to examine the associations of BP with concentric remodeling and different patterns of LV hypertrophy in separate models using normal geometry as a control. The race differences in odds ratios (ORs) for LV geometric patterns were tested by including the respective race–BP and race–covariate interaction terms in separate models. The SBP, DBP and covariates, except for gender, were standardized into Z scores with a mean of 0 and SD of 1 before logistic regression analyses to make the ORs comparable. The triglycerides and triglyceride/high-density lipoprotein cholesterol ratio were log-transformed to improve the normality of the distribution in the general linear models and logistic regression models; however, the mean values in the original scales are listed in Table 1 for descriptive purposes.
| Variable | Blacks | Whites | ||||||
|---|---|---|---|---|---|---|---|---|
| Normal (n = 230) | CR (n = 27) | EH (n = 54) | CH (n = 32) | Normal (n = 597) | EH (n = 71) | CH (n = 32) | CR (n = 80) | |
| Age (years) | 38 ± 5 | 39 ± 5 | 40 ± 4 ⁎ | 39 ± 5 | 39 ± 4 | 39 ± 5 | 39 ± 5 | 40 ± 3 |
| Gender (n) | ||||||||
| Men | 87 | 13 | 23 | 8 | 241 | 49 | 44 | 9 |
| Women | 143 | 14 | 31 | 24 † | 356 | 31 ⁎ | 27 | 23 † |
| Body mass index (kg/m 2 ) | 29 ± 7 | 29 ± 6 | 37 ± 9 ⁎ | 38 ± 10 ⁎ | 28 ± 6 | 29 ± 5 | 36 ± 7 ⁎ | 34 ± 6 ⁎ |
| Triglycerides (mg/dl) | 104 ± 67 | 86 ± 40 | 123 ± 111 | 115 ± 58 | 139 ± 105 | 157 ± 129 | 165 ± 122 | 169 ± 95 |
| High-density lipoprotein cholesterol (mg/dl) | 53 ± 15 | 54 ± 13 | 49 ± 12 † | 50 ± 13 | 49 ± 13 | 44 ± 11 | 42 ± 12 ⁎ | 44 ± 10 ⁎ |
| Triglyceride/high-density lipoprotein cholesterol ratio | 2.3 ± 2.2 | 1.7 ± 0.9 | 2.6 ± 2.1 | 2.6 ± 1.9 | 3.3 ± 3.2 | 4.2 ± 5.2 | 4.4 ± 3.8 † | 4.0 ± 2.4 |
| Low-density lipoprotein cholesterol (mg/dl) | 121 ± 35 | 109 ± 31 | 116 ± 46 | 122 ± 36 | 127 ± 33 | 127 ± 32 | 127 ± 31 | 135 ± 32 |
| Glucose (mg/dl) | 94 ± 37 | 85 ± 13 | 89 ± 20 | 107 ± 39 ⁎ | 87 ± 18 | 90 ± 26 | 101 ± 31 ⁎ | 100 ± 48 ⁎ |
| Systolic blood pressure (mm Hg) | 119 ± 15 | 121 ± 14 | 134 ± 19 ⁎ | 139 ± 19 ⁎ | 113 ± 12 | 113 ± 11 | 121 ± 13 ⁎ | 121 ± 15 ⁎ |
| Diastolic blood pressure (mm Hg) | 74 ± 11 | 74 ± 10 | 83 ± 12 ⁎ | 86 ± 13 ⁎ | 71 ± 9 | 71 ± 8 | 76 ± 8 ⁎ | 76 ± 9 ⁎ |
| Left ventricular mass index (g/m 2.7 ) | 33 ± 7 | 36 ± 7 † | 57 ± 8 ⁎ | 59 ± 13 ⁎ | 32 ± 8 | 36 ± 7 ⁎ | 55 ± 8 ⁎ | 55 ± 10 ⁎ |
| Relative wall thickness | 0.32 ± 0.05 | 0.46 ± 0.03 ⁎ | 0.35 ± 0.04 ⁎ | 0.47 ± 0.05 ⁎ | 0.32 ± 0.05 | 0.47 ± 0.05 ⁎ | 0.36 ± 0.05 ⁎ | 0.48 ± 0.06 ⁎ |
Results
Figure 1 shows the prevalence of the LV geometric patterns by race. The black patients had a greater prevalence of eccentric hypertrophy (15.7% vs 9.1%, p <0.001) and concentric hypertrophy (9.3% vs 4.1%, p <0.001) than the white patients. Furthermore, the blacks had a greater prevalence of hypertension than the whites (33.2% vs 15.1%, p <0.001). With respect to the overall average BP level by race groups, significant race differences in the BP mean levels were noted among those who were normotensive (SBP 111.1 mm Hg in whites and 115.1 mm Hg in blacks, p <0.001; DBP 75.1 mm Hg in whites and 76.6 mm Hg in blacks, p <0.001). Among those with hypertension, a significant race difference was noted in the SBP (135.7 mm Hg in whites and 143.8 mm Hg in blacks, p <0.001) but not in DBP (94.3 mm Hg in whites and 95.5 mm Hg in blacks, p = 0.355).
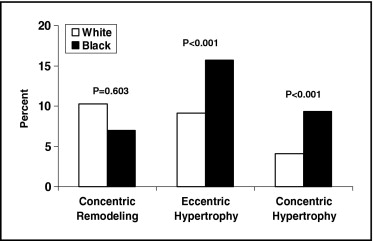
Table 1 lists the characteristics of the study variables by race and LV geometric patterns. Compared to the normal geometry group, those with eccentric and concentric hypertrophy showed significantly greater levels of body mass index (BMI), SBP, and DBP, adjusting for age and gender, in both blacks and whites. The mean BMI levels, lipid variables, glucose levels, and BP did not differ significantly between the normal geometry and concentric remodeling groups.
The association parameters (ORs) of BP with different LV geometric patterns derived from logistic regression models using the normal geometry as a control are listed in Table 2 . The SBP and DBP levels (Z scores) were significantly associated with eccentric hypertrophy and concentric hypertrophy in blacks. In contrast, only SBP was associated with concentric hypertrophy among the whites. The BP levels were not associated with concentric remodeling for both blacks and whites. The BMI showed significant and consistent associations with eccentric hypertrophy and concentric hypertrophy in blacks and whites, but not with concentric remodeling. Female gender was associated with a lower risk of concentric remodeling; however, women were more likely to have concentric hypertrophy, especially in black women (OR 5.91 to 7.07, p <0.01). With respect to race difference, the associations of SBP and DBP with eccentric and concentric hypertrophy were significantly stronger in the blacks than in the whites; the other study variables did not show race differences in the ORs.
| Variable | CR Versus Normal | EH Versus Normal | CH Versus Normal | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Whites | Blacks | p Value ⁎ | Whites | Blacks | p Value ⁎ | Whites | Blacks | p Value ⁎ | |
| Model 1 | |||||||||
| Age | 1.05 | 1.28 | 0.501 | 1.25 | 1.63 † | 0.398 | 1.59 † | 1.13 | 0.356 |
| Women | 0.43** | 0.58 | 0.537 | 0.73 | 1.24 | 0.382 | 3.06 † | 7.07 ‡ | 0.724 |
| Body mass index | 1.11 | 1.28 | 0.611 | 2.82 ‡ | 3.67 ‡ | 0.391 | 1.92 ‡ | 2.63 ‡ | 0.203 |
| Triglyceride/high-density lipoprotein cholesterol ratio | 1.10 | 0.63 | 0.077 | 1.04 | 1.13 | 0.838 | 1.11 | 0.93 | 0.795 |
| Low-density lipoprotein cholesterol | 0.95 | 0.63 | 0.088 | 0.75 † | 0.58 ‡ | 0.403 | 0.93 | 0.82 | 0.817 |
| Glucose | 1.12 | 0.77 | 0.214 | 1.21 | 0.48 | 0.077 | 1.31 † | 1.20 | 0.670 |
| Systolic blood pressure | 0.83 | 1.02 | 0.700 | 0.95 | 1.82 ‡ | 0.016 | 1.50 † | 3.74 ‡ | 0.007 |
| Model 2 | |||||||||
| Age | 1.04 | 1.32 | 0.484 | 1.27 | 1.66 † | 0.402 | 1.65 † | 1.16 | 0.267 |
| Women | 0.42 ‡ | 0.57 | 0.526 | 0.73 | 0.81 | 0.404 | 3.09 † | 5.91 ‡ | 0.713 |
| Body mass index | 1.08 | 1.35 | 0.607 | 2.95 ‡ | 3.36 ‡ | 0.447 | 2.06 ‡ | 2.49 ‡ | 0.353 |
| Triglyceride/high-density lipoprotein cholesterol ratio | 1.10 | 0.65 | 0.076 | 1.05 | 1.20 | 0.889 | 1.10 | 0.96 | 0.755 |
| Low-density lipoprotein cholesterol | 0.95 | 0.62 | 0.091 | 0.76 | 0.59 ‡ | 0.344 | 0.94 | 0.76 | 0.627 |
| Glucose | 1.11 | 0.77 | 0.211 | 1.22 | 0.47 | 0.065 | 1.33 † | 1.16 | 0.492 |
| Diastolic blood pressure | 0.90 | 0.83 | 0.601 | 0.84 | 1.62 ⁎ | 0.017 | 1.35 | 2.86 ‡ | 0.026 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


