Hypereosinophilic syndrome is characterized by unexplained hypereosinophilia involving different organ systems. The investigators present a patient diagnosed with hypereosinophilic syndrome in which cardiac magnetic resonance was pivotal in establishing the presence of cardiac involvement.
Case Description
A 77-year-old woman presented with 6 months of fatigue and malaise associated with diarrhea and weight loss (current weight 57 kg). Her heart was enlarged, and a third heart sound was heard at the apex. Transthoracic echocardiography showed a moderately dilated left ventricle with impaired systolic function, a moderate pericardial effusion, and an abnormal right ventricular (RV) apex with a hyperechogenic signal. The C-reactive protein level was 86 mg/L, and the eosinophil count was 3,810/μL (normal values <500/μL).
Cardiac magnetic resonance (CMR) demonstrated a dilated left ventricular cavity (indexed end-diastolic and end-systolic volumes 131 and 90 ml/m 2 , respectively), with an left ventricular ejection fraction of 30% and mild biatrial dilatation.
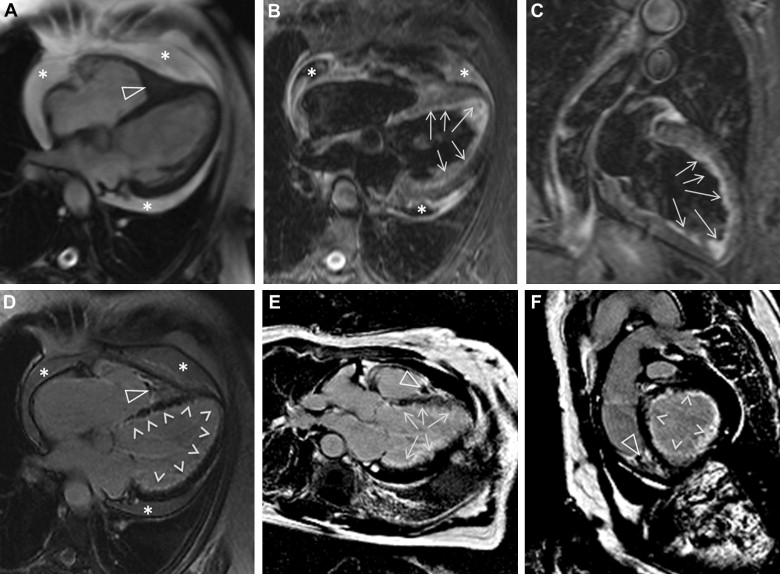
Myocardial tissue characterization was obtained using T1- and T2-weighted imaging. The latter sequence showed diffuse circumferential subendocardial high signal intensity in the midcavity and apical segments, suggesting active myocardial inflammation. T1-weighted imaging after contrast administration revealed diffuse circumferential endocardial late gadolinium enhancement of almost all LV and RV segments. An RV apical thrombus (0.7 × 0.7 cm 2 ) was also identified ( Figure 1 ).
Comments
Hypereosinophilic syndrome (HES) is a disease characterized by unexplained hypereosinophilia that can involve different organ systems. The main diagnostic criteria for HES include (1) persistent hypereosinophilia of 1,500 eosinophils/μL lasting >6 months, (2) no evidence of allergic, parasitic, or other cause associated with hypereosinophilia, and (3) evidence of organ damage (heart, nervous system, or bone marrow).
Cardiac involvement is found in about 60% of patients with HES, it is the major cause of mortality and morbidity in this syndrome, and it manifests as ventricular thickening, usually by fibrous tissue.
In our patient, CMR showed circumferential endocardial fibrosis after gadolinium contrast administration, which is pathognomonic of hypereosinophilia cardiac involvement. In addition, CMR showed acute myocardial edema with the same distribution and an intracavity thrombus at the RV apex, suggesting an active phase of the disease, supported also by the high level of plasmatic C-reactive protein in our patient. The left ventricular cavity was dilated, a feature rarely seen in HES cardiac involvement.
Echocardiography can identify cardiac involvement in 40% to 50% of patients with HES. There is an emerging role of CMR in these patients given its increased spatial resolution compared with echocardiography and its additional unique capability of noninvasive tissue characterization.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


