The investigators describe the occurrence of an episode of acute tako-tsubo cardiomyopathy in a 51-year-old woman, which was followed, only days later, by an episode of acute tako-tsubo cardiomyopathy in her 74-year-old mother. The mother and daughter had distinctly different left ventricular contraction patterns, yet the left anterior descending coronary artery distribution was similar, extending beyond the left ventricular apex in both women. In conclusion, this unusual scenario suggests a familial predisposition to tako-tsubo cardiomyopathy. Furthermore, the daughter’s event may have contributed to (or triggered) the tako-tsubo episode in her mother.
Tako-tsubo (stress) cardiomyopathy (TTC) is a typically reversible and recently recognized cardiomyopathy with acute onset, characterized by a distinctive left ventricular (LV) contraction profile and a predilection for middle-aged and older women, which is usually triggered by a stressful event. Indeed, a physically or an emotionally stressful event immediately precedes the abrupt development of acute heart failure in about 90% of patients with TTC. Although the pathophysiology of TTC is unknown, some evidence points to activation of the sympathetic nervous system with increased catecholamine levels as a disease element. Reports of familial TTC occurrence are rare but with substantial time intervals between TTC events in family members. In this report, we describe a TTC event in a mother that was likely influenced by TTC occurring in her daughter just days earlier.
Case Descriptions
A 51-year-old postmenopausal woman had an acute and reversible TTC event, triggered by physical exertion while hiking a mountain in the Utah desert during hot weather (altitude >5,000 ft, temperature ≥ 100°F). Only 18 days later, her 74-year-old mother also presented with acute and reversible TTC, apparently triggered by psychological stress attributed to her daughter’s TTC event, as well as the death (from cancer) of another 54-year-old daughter 4 months earlier.
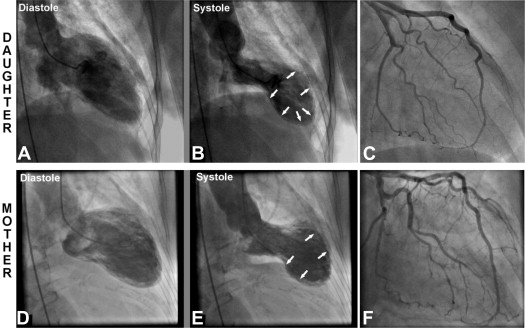
The angiographic appearance of the left ventricle in systole during the 2 TTC events differed considerably in the related patients ( Figure 1 ). The daughter showed the most typical TTC pattern, with LV apical ballooning, while the mother demonstrated the less common TTC pattern of mid-LV ballooning with preserved apical contraction. Despite disparate LV apical contraction patterns, the left anterior descending coronary artery (LAD), without obstructive atherosclerosis, showed a similar distribution, extending beyond the LV apex in the daughter and her mother.
Comments
We present a unique clinical scenario in which 2 TTC events occurred in first-degree relatives only days apart. TTC is an uncommon acute cardiomyopathy, and familial occurrence, as reported here, is rare. However, genetic investigations in TTC are limited. Polymorphism frequencies of the β 1 -adrenergic receptor (amino acid positions 389 and 49) and α 2c -adrenergic receptor (deletion 322-325) are not significantly different in patients with TTC compared with female controls. Furthermore, adrenergic receptor gene mutations were not evident in a mother and daughter with TTC. In contrast, a small study reported that the rs17098707 polymorphism of the G protein–coupled receptor kinase 5 gene is present at a significantly higher frequency in patients with TTC, providing preliminary evidence for a genetic influence in TTC.
Nevertheless, the short time interval between the daughter’s and mother’s TTC events (<3 weeks) suggests to us that these occurrences cannot likely be explained on the basis of simple coincidence. Rather, our observation suggests a susceptibility to TTC, which presently remains undefined.
Although the mother and daughter reported here had distinctly different LV contraction patterns, the LAD distribution was similar (extending beyond the LV apex in both women). Transient vasospasm, atheroembolism, thrombosis, and myocardial bridging involving the LAD have all been proposed as possible mechanisms for TTC, each of which would lead to ischemia in the LAD-perfused myocardium. The disparate LV contraction patterns evident in these 2 related patients, despite similar LAD anatomy, suggest that TTC is initiated by mechanisms independent of epicardial coronary artery distribution. This concept is consistent with reports that recurrent TTC events in the same patient may be associated with different “ballooning” patterns.
In the unusual TTC scenario presented here, a daughter’s TTC event appears to have contributed to (or triggered) a TTC episode in her mother only days later, with a different LV contraction pattern.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


