24 Cutting Balloon Angioplasty The aim of this procedure is a less traumatic dilatation of coronary stenoses by defined longitudinal incision of the atheroma using three or four integrated microblades (also called microatherotomes), or superimposed wires that are mounted on a balloon. Theoretically, this should limit the dilatation-induced vessel injury and thus also the reactive processes that promote the development of restenosis to the site of incision. Furthermore, recoil should be reduced after dilatation. This all should decrease the restenosis rate (Fig. 24.1). Another advantage is that these balloons do not slip during inflation, which is especially important for focal in-stent stenoses. There is extensive data for cutting balloons available from clinical studies. The primary indications are The procedure is not suitable for
 Basics
Basics
Cutting Balloon
 Indications and Contraindications
Indications and Contraindications
 In-stent restenoses, preferably focal
In-stent restenoses, preferably focal
 Stenoses in smaller vessels (< 3.0 mm)
Stenoses in smaller vessels (< 3.0 mm)
 Ostial stenoses
Ostial stenoses
 Bifurcation stenoses, origin of the side branch
Bifurcation stenoses, origin of the side branch
 Stenoses < 20 mm
Stenoses < 20 mm
 Visible severe calcifications
Visible severe calcifications
 Very tortuous vessels
Very tortuous vessels
 Stenoses in bends > 45°
Stenoses in bends > 45°
 Long stenoses > 20 mm
Long stenoses > 20 mm
 Total occlusion
Total occlusion
 Instrumentarium
Instrumentarium
Description of balloon (Fig. 24.2):

Balloon system: | Rapid-exchange; noncompliant balloon; hydrophilic coating |
Balloon diameter: | 2.00 to 4.00 mm (0.25-mm increments) |
Guidewire: | Max. 0.014 in. |
Guiding catheter: | 6F |
Length of the atherotomes: | 6, 10 or 15 mm |
Number of atherotomes: | 3 (up to 3.25 mm balloon diameter) |
Working height of the atherotomes: | 0.005 in (0.127 mm) |
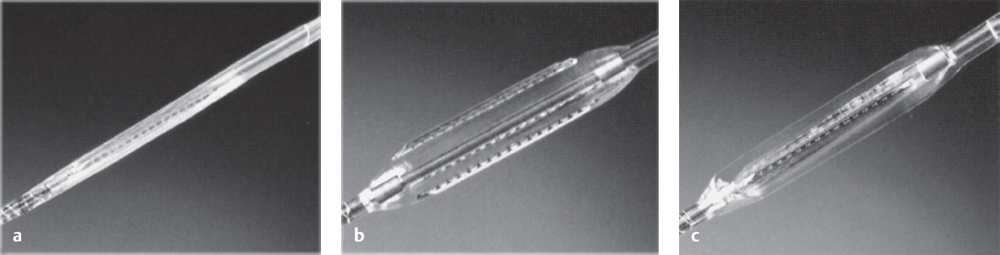
Fig. 24.2 a–c Cutting balloon.
a Prepared balloon.
b Expanded balloon.
c After deflation of the balloon.
 Procedure
Procedure
Special Patient Preparation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


