Although percutaneous coronary angioplasty became widely accepted after being first performed by Greuntzig in 1977, abrupt in-lab closure and late restenosis remained problematic. To combat these issues, several varieties of self-expanding and balloon expandable stents were developed. In 1987, Sigwart et al. reported the first coronary stent experience in humans (1). Self-expanding Wallstents were placed in 19 patients who presented with coronary artery restenosis or abrupt closure. Although short-term results were favorable, follow-up showed frequent stent thrombosis and restenosis (2).
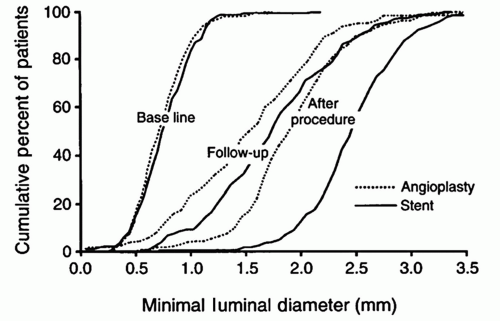
Subsequently, in 1993, the balloon expandable Gianturco-Roubin stent was the first coronary stent approved by the U.S. Food and Drug Administration (FDA) for the treatment of acute vessel closure. Current-generation slotted tube, balloon expandable stents are based on the original Palmaz-Schatz platform. The pivotal BENESTENT and STRESS studies showed significantly lower restenosis rates in native coronary stented lesions compared with those treated with balloon angioplasty (3, 4) (Fig. 14-1). The Palmaz-Schatz stent was approved for clinical use by the FDA in 1994. Although Palmaz-Schatz stents effectively eliminated acute in-lab vessel closure, they were associated with increased intimal hyperplasia, resulting in high restenosis rates, especially in small vessels or long lesions.
The use of intravascular ultrasound (IVUS) documented that early stent implantation techniques were inadequate to fully expand these stents (5). High-pressure balloon postdilation and the introduction of dual antiplatelet agent therapy in the mid-1990s led the way to widespread use of stents in most lesions (6, 7). Second- and third-generation slotted tube stents improved on strut thickness, trackability, restenosis rates, and range of available sizes. Not until drug-eluting coatings were added did restenosis rates fall significantly.
The prototype drug-eluting stent (DES) (Cypher, Cordis) was approved by FDA in 2003 after the pivotal Sirius Trial showed significantly lower restenosis rates compared with those of an uncovered (bare-metal) stent (BMS) (8). Subsequently, many different drug and polymer coatings have been studied (9, 10 and 11). More importantly, the use of stents for increasingly complex lesion and patient subsets has been investigated. This chapter highlights some of the important milestones in the development of stents and our current understanding regarding stent use in various populations.
FIGURE 14-1 Primary outcome data from the STRESS trial. The minimal lesion lumen diameter at baseline, immediately after stent placement or angioplasty and at follow-up. (From: Fischman, et al. N Engl J Med. 1994;331:496-501, with permission.)
MEASURES OF DEVICE AND PROCEDURAL SUCCESS
The majority of studies investigating stent effectiveness have employed quantitative coronary angiography. By measuring lesionlumen diameter prior to (pre) and following implant (post) and at late follow-up (late), several important measures can be calculated:
Acute gain = post — pre minimal lesion diameter
Late loss = post — late minimal lesion diameter
These measures relate to the physical performance of the stent. In general, the greater the acute gain is, the greater the late loss will be. Angiographic restenosis at late follow-up is typically defined as a late lesion diameter stenosis >50%. This is often displayed as a cumulative frequency distribution curve (12). Similar measures can be obtained using IVUS, which has often been included in a subset of stent trial patients.
It is also important to understand measures of clinical outcome. This is generally defined as the rate of clinically (or ischemia) driven repeat revascularization (either by repeat intervention or by bypass) at a time ranging from 6 to 12 months after the index procedure. Major adverse cardiac events (MACE) are classically defined as death, Q-wave myocardial infarction (MI), or revascularization. Commonly used endpoints include the following:
Target lesion revascularization (TLR): Any repeat revascularization of the original lesion, which includes the stented region and 5 mm proximal and distal to the stent.
Target vessel revascularization (TVR): Any repeat revascularization involving the previously treated vessel.
Target vessel failure (TVF): Combination of TVR and MACE.
COMPARISON OF BMS AND BALLOON ANGIOPLASTY
The pivotal trials of stent use are important to understand as a basis for current practice. The STRESS study was a randomized controlled trial that assigned 401 patients to Palmaz-Schatz stent or balloon angioplasty (4). The primary endpoint was angiographic evidence of restenosis, defined as at least 50% stenosis on the 6-month follow-up angiogram. The patients who underwent stenting had a higher rate of procedural success (96.1% vs. 89.1%; p = 0.011), and a larger acute gain (1.72 ± 0.46 mm vs. 1.23 ± 0.48 mm; p < 0.001). At 6 months, the patients who received stents had lower rate of restenosis (31.6% vs. 42.1%; p = 0.046) and had larger net gain (0.98 ± 0.62 mm vs. 0.80 ± 0.63 mm; p = 0.01), but had higher late loss (0.74 ± 0.58 mm vs. 0.38 ± 0.66 mm; p < 0.001). There was no difference in late clinical outcomes, but there was a trend toward less TVR (10.2% vs. 15.4%; p = 0.06) in the stented patients.
BENESTENT was a multicenter randomized controlled trial performed in Europe (3). A total of 520 patients with stable angina and a single coronary artery lesion were randomly assigned to either Palmaz-Schatz stent or balloon angioplasty. The primary clinical endpoint was TVF, defined as death, cerebrovascular accident, MI, and TVR. The primary angiographic endpoint was the minimal luminal diameter at follow-up. Patients who received stents had fewer primary clinical endpoints (20.1% vs. 29.6%; relative risk [RR]: 0.68; 95% confidence interval [CI]: 0.50-0.92). The difference in clinical event rates was explained mainly by a reduced TVR (13.5% vs. 23.3%; RR: 0.58; 95% CI: 0.40-0.85). The patients who received stents also had less angiographic restenosis (22% vs. 32%; p = 0.02), larger acute gain (1.40 ± 0.44 mm vs. 0.97 ± 0.39 mm; p < 0.01), but also greater late loss (0.65 ± 0.57 mm vs. 0.32 ± 0.47 mm; p < 0.01). There was a trend toward larger net gain in the stent-treated group (0.75 ± 0.66 mm vs. 0.65 ± 0.59 mm; p = 0.09).
STENT THROMBOSIS
Stent thrombosis is a rare but usually catastrophic event, frequently associated with a large MI or death. In BMS clinical trials, stent thrombosis rates were <1% with the use of dual antiplatelet therapy and high-pressure postdilation, although higher rates (2%-3%) were reported when more complex patients or lesions were treated. Most events occurred within the first few days. Initial reports of DES clinical trials showed no increased risk for stent thrombosis during early and mid-term follow-up compared with BMS, but concerns were heightened by reports of increased rates of very late thrombosis occurring beyond the recommended duration of dual antiplatelet therapy (13).
Definitions of stent thrombosis in clinical trials of DES have not been uniform. In an effort to standardize reporting, the Academic Research Consortium (ARC) has produced a common definition set, which is now universally accepted (Table 14-1). Stent thrombosis will be discussed along with other clinical outcomes in the comparisons to follow. The generally accepted risk factors for stent thrombosis are listed in Table 14-2.
TABLE 14-1 Academic Research Consortium (ARC) Definition of Stent Thrombosis
Definite stent thrombosis:
Angiographic confirmation: the presence of thrombus that originates in the stent or in the 5 mm proximal or distal to the stent and presence of at least 1 of the following criteria within a 48-hour time window
Acute onset of ischemic symptoms at rest
New ischemic EKG changes
Typical rise and fall in cardiac biomarkers
Pathological confirmation
Probable stent thrombosis:
Unexplained death within the first 30 days
Target vessel infarction without angiographic confirmation
Possible stent thrombosis: unexplained death after 30 days
Stent thrombosis timing:
Acute stent thrombosis: 0 to 24 hours after stent implantation
Subacute stent thrombosis: >24 hours to 30 days after stent
implantation
Late stent thrombosis: >30 days to 1 year after stent implantation
Very late stent thrombosis: >1 year after stent implantation.
TABLE 14-2 Factors Associated with an Increased Risk of Drug-Eluting Stent Thrombosis (37)
Patient
Dual antiplatelet discontinuation
Diabetes
Acute coronary syndrome/myocardial infarction
Low ejection fraction
Renal failure
Lesion
Bifurcation
Longer stent length
Residual dissection
Small stent diameter and/or severe under expansion
Stent malapposition
COMPARISON OF DES AND BMS
First-Generation DES
Although BMS have lower restenosis rates compared with balloon angioplasty, they have greater late loss from the neointimal hyperplastic response to vascular injury. DES were developed specifically to reduce this neointimal hyperplasia by inhibiting cellular proliferation. DES comprise three interrelated components: a metallic stent scaffold, a drug-containing coating, and a specific antiproliferative drug. For each DES variety, a general knowledge of these three components is important.
The prototype DES is the sirolimus-eluting stent (Cypher, Cordis). The scaffold is a slotted tube design made of 316 L stainless steel. A nonerodable polymer coating is adhered to the entire surface (luminal and abluminal) of the stent. The antiproliferative agent used is sirolimus (rapamycin). Sirolimus is a macrocyclic lactone produced by Streptomyces hygroscopicus, a bacteria that was isolated from an Easter Island soil sample. Sirolimus was initially found to have antifungal properties (14); however, it has been more extensively used for its antiinflammatory and antiproliferative properties. Sirolimus binds to FK-Binding Protein 12 (FKBP-12). The resulting complex inhibits the activation of the mammalian target of rapamycin (mTOR), leading to inhibition of cell cycle progression from G1 to the S phase (15).
SIRIUS was the pivotal study for the Cypher stent (8). It was a randomized, double-blind trial comparing sirolimus-eluting stents (SES) (Cypher, Cordis) and standard BMS (Bx Velocity, Cordis) in 1,058 patients at 53 centers in the United States who had a newly diagnosed lesion in a native coronary artery. Inclusion criteria were a lesion resulting in a stenosis of 51% to 99%, measuring 15 to 30 mm in length. Stents were available in 15-mm length and 2.5-, 3.0-, and 3.5-mm diameters. Clopidogrel was given for 3 months. Follow-up clinical information was obtained at 1, 3, 6, and 9 months. Coronary angiograms were obtained at baseline, at the completion of the procedure, and at 8-month follow-up. IVUS was performed after the procedure and at 8 months in a subset of 250 patients. The primary endpoint was TVF. The rate of TVF was reduced from 21.0% with BMS to 8.6% with SES (p < 0.001). The reduction was driven largely by a decrease in TVR (16.6% BMS vs. 4.1% SES; p < 0.001). Neointimal hyperplasia within the stent was also decreased in the group that received SES, as assessed by quantitative angiography and IVUS (late loss: 1.00 ± 0.70 mm BMS vs. 0.17 ± 0.45 mm SES; p < 0.001).
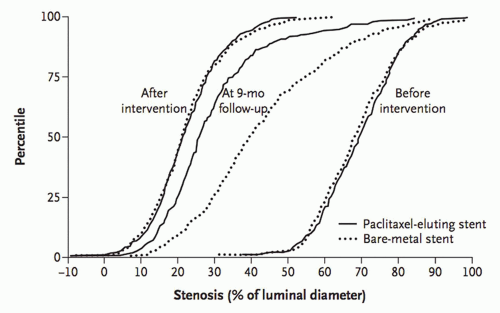
FIGURE 14-2 Restenosis data from the TAXUS IV trial. Cumulative frequency distribution curves for lesion percent diameter stenosis before, immediately after intervention, and at 9-month follow-up. (From: Stone, et al. N Engl J Med. 2004;350:221-231, with permission.)
The TAXUS stent was the second DES approved in the United States. This paclitaxel-eluting stent (PES) (TAXUS, Boston Scientific, Natick, MA) is also made of 316 L stainless steel coated with a polymer carrier loaded with 1µg/mm2 paclitaxel in a slow release formulation. In 1962, samples of the plant Taxus brevifolia were collected and studied. One compound from the plant was named Taxol (16
Only gold members can continue reading. Log In or Register to continue