Coronary Artery Anomalies
Anomalies of the coronary arteries are rare and include left coronary artery origin from the pulmonary artery, coronary artery fistula, and aberrant origin of the left or right coronary artery with subsequent coursing between the great vessels.
Anomalous Left Coronary Artery from the Pulmonary Artery
Origin of the left coronary artery from the pulmonary artery is the most common congenital coronary artery anomaly and occurs in 1 of every 300,000 livebirths. This anomaly is compatible with in utero life because of the presence of relatively high pulmonary artery pressure and oxygen saturation. However, over the first 1 to 3 months of life as the pulmonary vascular resistance decreases, the flow into the left coronary artery decreases, resulting in inadequate coronary perfusion. This may lead to progressive dilatation of the left ventricle, myocardial infarction, and secondary mitral regurgitation. Lack of adequate perfusion stimulates the development of collateral circulation from the right coronary artery to the left system. Significant left-to-right shunting secondary to run off from these collateral vessels into the pulmonary artery may occur. The clinical course of the patient depends on the relative dominance of the right and left coronary arteries and the rapidity and extent of collateral development.
Surgical Anatomy
The ostium of the anomalous left main coronary artery may be located anywhere in the main pulmonary artery or the proximal right or left pulmonary artery. Most commonly, it is found leftward in the posterior sinus of the pulmonary root (the sinus facing the aortic sinus, which normally gives rise to the left main coronary artery).
Incision
An anomalous left coronary artery from the pulmonary artery is best approached through a median sternotomy with standard cardiopulmonary bypass.
Technique
Before commencing cardiopulmonary bypass, the right and left pulmonary arteries are dissected and encircled with snares. High cannulation of the ascending aorta is performed and a single venous cannula is used. Immediately after starting cardiopulmonary bypass, the snares around the pulmonary arteries are tightened. A vent is placed into the left ventricle through the right superior pulmonary vein (see Chapter 4). Cooling to 28°C is carried out, and antegrade cardioplegic solution is delivered into the aortic root after the cross-clamp is applied.
A transverse incision is made on the pulmonary artery just above the sinotubular ridge. Snares around the right and left pulmonary arteries are removed. The ostium of the anomalous coronary artery is identified. It is often possible to administer cardioplegic solution directly into this vessel with an appropriately sized olive-tipped catheter for optimal myocardial protection. The main pulmonary artery is now transected, and the ostium of the anomalous left coronary artery is excised with a generous margin of tissue as a button or a U-shaped flap from within the pulmonary sinus (Fig. 32-1).
The anterior edge of the pulmonary artery root is pulled downward with a traction suture. This maneuver will improve visualization of the anomalous left coronary artery. It is mobilized and dissected free from the surrounding tissues with a low-current electrocautery. The coronary artery, now well mobilized, is brought up toward the left posterior aspect of the ascending aorta (Fig. 32-2). A small vertical or transverse incision is made on the aorta to identify the precise location of the aortic leaflets and commissures. Under direct vision, a slit is made on the posterior aspect of the aortic wall, taking meticulous care not to injure the aortic valve components. The opening is then enlarged appropriately to accommodate the left coronary using a 4-mm coronary aortic punch. The left coronary button or flap is then anastomosed to the aortic opening with 6-0 or 7-0 Prolene suture. The aortotomy is closed with continuous 6-0 Prolene suture. The defect in the pulmonary root is patched with a piece of autologous pericardium using a running 6-0 or 7-0 Prolene suture. The pulmonary root is then reattached to the pulmonary artery confluence with a continuous suture of 5-0 Prolene (Fig. 32-3).
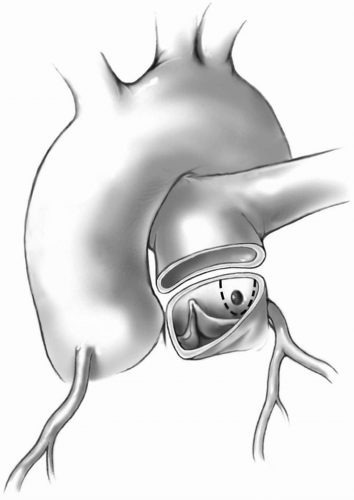 FIG 32-1. Transected pulmonary artery. Dotted line demonstrates excision of the left main coronary artery. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


