Before performing percutaneous coronary interventions (PCI), coronary angiography should establish the precise lesion length, morphology, and degree of calcification (or thrombus), as well as the relationship to side branches and their associated ostial involvement with atherosclerosis. Knowledge of optimal angiographic projections will assist in guide catheter selection, visualizing the target vessel course and angle for optimal treatment, the distribution of collateral supply, and estimating the true (maximally vasodilated) dimensions of PCI artery.
Optimal definition of the ostial and proximal coronary segment is critical to guide PCI catheter selection. Assessment of calcium using angiography is less reliable than using intravascular ultrasound (IVUS) imaging, but still serves a useful purpose in determining the need for rotational atherectomy. Coronary angiography defines the risks associated with the procedure and demonstrates a successful intervention.
For chronic total vessel occlusion PCI feasibility, the distal vessel should be visualized as clearly as possible. This may require the simultaneous injection of collateral supply arteries with cineangiography of sufficient duration to visualize late collateral vessel filling and the length of the occluded segment.
Radiation exposure is higher in PCI than in diagnostic procedures (1, 2 and 3). Continued awareness of the inverse square law of radiation propagation will reduce the exposure to patient, operators, and the cath lab team. Obtaining quality images should not necessitate increasing the ordinary procedural radiation exposure to either the patient or the catheterization personnel.
COMMON ANGIOGRAPHIC VIEWS FOR PCI
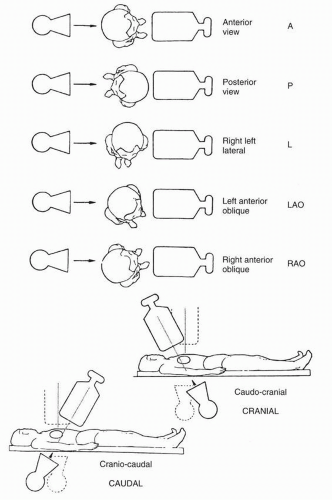
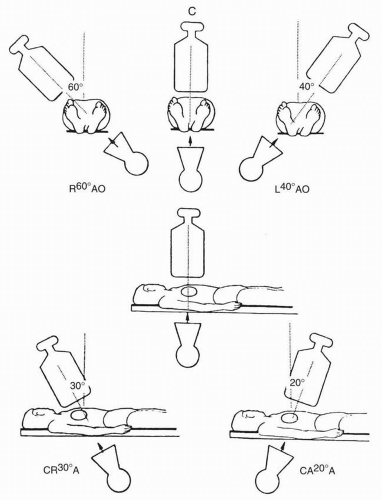
The nomenclature for angiographic views will be reviewed briefly here, emphasizing the interventionalist’s thinking for visualizing anatomy for appropriate revascularization. Classic terminology for angiographic projections with regard to left (LAO) and right anterior oblique (RAO), cranial and caudal angulation, and lateral projections remains as defined in previous discussions of diagnostic coronary angiography (4, 5).
Anteroposterior Imaging
The image intensifier is directly over the patient, with the beam perpendicular to the patient lying flat on the x-ray table (Figs. 11-1 and 11-2). The anteroposterior (AP) view or shallow RAO displays the left main coronary artery (LMCA) in its entire perpendicular length. In this view, the branches of the left anterior descending (LAD) and left circumflex coronary arteries branches overlap. In patients with acute coronary syndromes, starting with this view to exclude left main stenosis will facilitate PCI. The AP cranial view is also excellent for visualizing the entire LAD with septals moving to the left (on screen) and diagonals to the right, thus helping wire placement.
RAO Imaging
The RAO caudal view shows the LMCA bifurcation with the origin and course of the circumflex/obtuse marginals, ramus intermediate branch, and proximal LAD segment. The LAD beyond the proximal segment is often obscured by overlapped diagonals. The RAO cranial or AP cranial views are used to open the diagonals along the mid- and distal LAD. The diagonal branches are projected upward.
For the right coronary artery (RCA), the RAO view shows the mid-RCA and the length of the posterior descending artery and posterolateral branches. Posterior descending artery (PDA) septals may show an occluded LAD via collaterals. The posterolateral branches overlap and may be best displayed with cranial angulation.
FIGURE 11-1 Nomenclature for angiographic views. (Modified from: Paulin S. Cathet Cardiovasc Diagn. 1981;7:341, with permission.)
FIGURE 11-2 Diagrammatic view of image intensifier for common angiographic projections.
Left Anterior Oblique Imaging
The LAO cranial view shows a foreshortened LMCA and the full course of the LAD. Septal and diagonal branches are separated clearly. The circumflex and marginals are foreshortened and overlapped. Cranial angulation tilts the LMCA down and permits visualization of the LAD/circumflex bifurcation.
For the RCA, the LAO cranial view shows the origin of the artery, its entire length, and the posterior descending artery bifurcation (crux). Cranial angulation tilts the posterior descending artery down to reduce foreshortening.
The LAO caudal view (“spider” view) shows a foreshortened LMCA, but excellent visualization of the bifurcation of the circumflex and LAD. Proximal and mid-portions of the circumflex and the origins of obtuse marginal branches are well seen. The LAD is markedly foreshortened in this view.
A left lateral view shows the mid- and distal LAD best. This view is best to see coronary artery bypass graft (CABG) conduit anastomosis to the LAD. The LAD and circumflex are well separated. Diagonals usually overlap. The course of the (ramus) intermediate branch is also well visualized.
For the RCA, the lateral view also shows the origin (especially in those with more anteriorly oriented orifices) and the mid-RCA well. The posterior descending artery and posterolateral branches are foreshortened.
Angulations for Saphenous Bypass Grafts
Coronary artery saphenous vein grafts are visualized in at least two views (LAO and RAO). It is important to show the aortic anastomosis, the body of the graft, and the distal anastomosis. The distal runoff and continued flow or collateral channels are also critical. The graft vessel anastomosis is best seen in the view that depicts the native vessel best (Table 11-1). The graft views can be summarized as follows:
RCA graft: LAO cranial/RAO and lateral
LAD graft (or internal mammary artery): lateral, RAO cranial, LAO cranial, and AP (the lateral view is especially useful to visualize the anastomosis to the LAD)
Circumflex (and obtuse marginals) grafts: LAO and RAO caudal
TABLE 11-1 Recommended “Key” Angiographic View for Specific Coronary Artery Segments
AP, anteroposterior; LAD, left anterior descending artery; LAO left anterior oblique; PDA, posterior descending artery (from RCA); RAO, right anterior oblique; RCA, right coronary artery.a Horizontal hearts. From: Kern MJ, ed. The cardiac catheterization handbook, St Louis, MO, Mosby, 1995: 286.
Angiographic TIMI Classification of Blood Flow
The Thrombolysis in Myocardial Infarction (TIMI) group’s system of flow grading has been used to assess, in a qualitative fashion, the degree of perfusion before and after thrombolysis or angioplasty in patients with acute myocardial infarction. Table 11-2 provides descriptions used to assign TIMI flow grades.
Classification of Distal Angiographic Contrast Runoff
The distal runoff is classified into four stages (also known as TIMI grade):
Normal distal runoff (TIMI 3)
Good distal runoff (TIMI 2)
Poor distal runoff (TIMI 1)
Absence of distal runoff (TIMI 0).
TIMI flow grades of 0 to 3 have become a standard description of coronary blood flow in clinical trials. TIMI flow grade of 3 has been associated with improved clinical outcomes.
TIMI Frame Count
Contrast runoff can be performed quantitatively by using cine frame counts. The method uses cineangiography with 6F catheters and filming at 30 frames/s. The number of cine frames from the introduction of dye in the coronary artery to a predetermined distal landmark is counted. The TIMI frame count (TFC) for each major vessel is thus standardized according to specific distal landmarks (6).
TABLE 11-2 Thrombolysis in Myocardial Infarction (TIMI) Flow: Grade and Blush Scores
TIMI Flow Grade
Description
Grade 3
Anterograde flow into the terminal coronary
(complete
artery segment through a stenosis is as
reperfusion)
prompt as anterograde flow into a comparable segment proximal to the stenosis. Contrast material clears as rapidly from the distal segment as from an uninvolved, more proximal segment
Grade 2
Contrast material flows through the stenosis to
(partial
opacify the terminal artery segment. However,
reperfusion)
contrast enters the terminal segment perceptibly more slowly than more proximal segments. Alternatively, contrast material clears from a segment distal to a stenosis noticeably more slowly than from a comparable segment not preceded by a significant stenosis
Grade 1
A small amount of contrast flows through the
(penetration with minimal perfusion)
stenosis, but fails to fully opacify the artery beyond
Grade 0
There is no contrast flow through the stenosis
(no perfusion)
Myocardial Blush Grade 0 No myocardial blush or contrast density. Myocardial blush persisted (“staining”). 1 Minimal myocardial blush or contrast density. 2 Moderate myocardial blush or contrast density but less than that obtained during angiography of a contralateral or ipsilateral noninfarct-related coronary artery. 3 Normal myocardial blush or contrast density, comparable with that obtained during angiography of a contralateral or ipsilateral noninfarct-related coronary artery Modified from: Sheehan F, et al. Circulation. 1987;72:817-829, with permission.
Typically, a normal contrast frame count reflecting normal flow is 24 ±10 frames. The TFC can further be corrected for the length of the LAD. The TFC in the LAD requires normalization or correction for comparing the two other major arteries. This is called corrected TFC (CTFC). High TFC (i.e., slow blood flow) may be associated with microvascular dysfunction despite an open epicardial artery. A CTFC of <20 frames has been associated with a low risk for adverse events in patients following myocardial infarction. The TFC method provides valuable information relative to clinical response after coronary intervention.
TIMI Myocardial Blush Grades
Washout of contrast from the microvasculature in the acute infarction patient is coupled with prognosis. Improved blush scores indicate a larger amount of myocardial salvage, whereas failure to improve the Myocardial Blush Grades (MBG) suggests microvascular dysfunction or occlusion. The MBG scoring system is shown in Table 11-2.
Angiographic Classification of Collateral Flow
Collateral flow can be seen and classified angiographically. The late opacification of a totally or subtotally (99%) occluded vessel through antegrade or retrograde channels will assist in correct guidewire placement, lesion localization, and a successful procedure. The collateral circulation is graded angiographically as established by Rentrop (12):
Grade 0: No collateral branches seen.
Grade 1: Very weak (ghost-like) opacification.
Grade 2: Opacified segment is less dense than the source vessel and filling slowly
Grade 3: Opacified segment is as dense as the source vessel and filling rapidly.
Only gold members can continue reading. Log In or Register to continue