Studies have shown an association between the presence of a patent foramen ovale (PFO) and cryptogenic stroke (CS) in patients aged <55 years. In addition, protruding atheromatous plaques in the ascending aorta and aortic arch are an independent risk factor for ischemic stroke in patients aged ≥55 years. The aim of this study was to determine the association of CS in the 2 age groups with PFO and with atheromatous plaques in the ascending aorta and in the aortic arch. Transesophageal echocardiograms in 229 patients evaluated for CS were compared to those in 314 patients evaluated for cardiac disease other than PFO with no histories of stroke (the control group). The prevalence of PFO and the presence of complex atheromatous plaques in the ascending aorta and aortic arch were determined in all patients and compared between the CS and control patients in the 2 age groups. The prevalence of PFO was significantly higher in patients with CS than in control patients among those aged <55 years (31 of 114 [27%] vs 24 of 171 [14%], p = 0.006) and those aged ≥55 years (28 of 115 [24%] vs 21 of 143 [15%], p = 0.049). The incidence of atrial septal aneurysm was similar in the 2 groups irrespective of patient age, as was the prevalence of complex atheromatous plaques. Multivariate analysis showed that PFO was independently associated with CS, irrespective of patient age (<55 years: odds ratio 2.4, 95% confidence interval 1.3 to 4.5, p = 0.01; ≥55 years: odds ratio 1.9, 95% confidence interval 1.1 to 3.5, p = 0.03). In conclusion, PFO was significantly associated with CS in younger (aged <55 years) and older (aged ≥55 years) patients. Atrial septal aneurysm and complex atheromas in the ascending aorta and aortic arch do not appear to be associated with CS.
The underlying mechanisms of stroke are heterogenous and thus represent a diagnostic challenge. Approximately 40% of strokes are cryptogenic. Two areas of focused interest have been the association of cryptogenic stroke with patent foramen ovale (PFO) and the relation of cryptogenic stroke with aortic atherosclerosis. Previous studies have shown a significant association between cryptogenic stroke and PFO, particularly in patients aged <55 years. As a result, most previous studies have focused on this age group, and the relation between cryptogenic stroke and PFO has not been extensively studied in patients aged ≥55 years. Although some studies have shown that protruding atheromatous plaques in the ascending aorta and aortic arch are an independent risk factor for ischemic stroke in patients aged ≥55 years, whether aortic atherosclerosis identified by transesophageal echocardiography (TEE) is a risk marker for cryptogenic stroke remains unclear. The purposes of this study were, in a series of patients with cryptogenic stroke who underwent TEE as part of their evaluation, (1) to confirm the association, if any, between cryptogenic stroke and PFO in patients aged ≥55 years and (2) to determine the association, if any, between cryptogenic stroke and protruding, complex atheromatous disease in the ascending aorta and aortic arch in patients aged <55 years and those aged ≥55 years.
Methods
From August 2006 to July 2008, 1,112 patients underwent TEE at the Pauley Heart Center at the Virginia Commonwealth University Hospitals (Richmond, Virginia). Patients with histories of unexplained stroke who underwent TEE for a possible cardiac source of embolization were retrospectively reviewed. After the exclusion of patients with other possible cardiac causes, a total of 229 patients with cryptogenic stroke, including 15 patients with transient ischemic attacks, were matched with 314 control patients on the basis of age and gender who underwent TEE during the same period for cardiac indications other than embolic symptoms; these patients served as a control group. Indications for TEE in the control patients included the following: before cardioversion for atrial arrhythmias and assessment of valve disease and for suspected endocarditis. The study protocol was approved by the institutional review board of the Virginia Commonwealth University School of Medicine.
The diagnosis of stroke was defined as a new onset of a neurologic deficit of >24 hours in duration. All patients with stroke underwent brain computed tomographic or magnetic resonance imaging scans, carotid arterial duplex Doppler examinations, and laboratory studies. Patients were categorized into 5 major stroke subtypes on the basis of possible underlying pathophysiologic mechanisms as defined by the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria: large artery atherosclerosis, cardioembolism, small-vessel occlusion, stroke of other determined origin, or stroke of undetermined origin. After a complete workup, patients with no identifiable causes of stroke were diagnosed as having cryptogenic stroke.
Risk factors for stroke were obtained by medical record review in the stroke and the control patients. They included age, gender, race, hypertension, diabetes mellitus, dyslipidemia (total cholesterol >200 mg/dl or receiving treatment for cholesterol reduction), documented coronary artery disease, and a history of smoking.
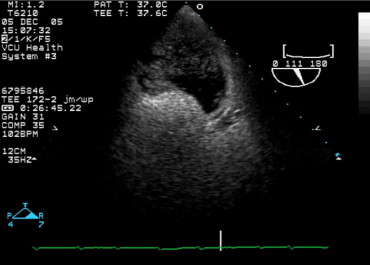
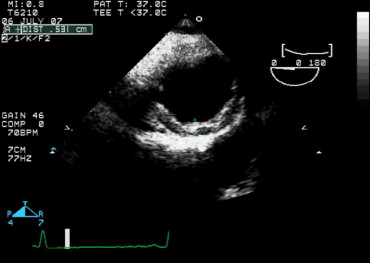
Patients underwent TEE using a multiplane probe with a Sonos 5500 system (Philips Medical Systems, Andover, Massachusetts). The presence of a PFO during TEE was determined by the intravenous injection of agitated saline in the bicaval view (approximately 90° to 120°), the aortic short-axis view, and the 4-chamber view. A PFO was diagnosed after saline injection when ≥4 microbubbles were observed early to transit the interatrial septum into the left atrium either spontaneously or during a provocative maneuver ( Figure 1 ) . An atrial septal aneurysm was identified when the excursion of an abnormally mobile atrial septum was >10 mm. Atherosclerosis was visualized during TEE in the ascending aorta, the aortic arch, and the descending thoracic and upper abdominal aorta and was defined as complex if there was protruding atheromatous plaque of >4-mm thickness, mobile debris, or plaque ulceration ( Figures 2 and 3 ) .

Results are expressed as mean ± SD. The prevalence of PFO and atherosclerosis was compared in patients with cryptogenic stroke and in control patients aged <55 years and ≥55 years. Pearson’s chi-square analysis was used to compare the discrete variables among groups. A p value <0.05 was considered statistically significant. Multivariate logistic regression analysis was used to test the association between PFO and atherosclerosis and cryptogenic stroke after entering age, gender, race, hypertension, diabetes mellitus, hypercholesterolemia, coronary artery disease, and history of smoking into the statistical model. SPSS version 14.0 (SPSS, Inc., Chicago, Illinois) was used for all analyses.
Results
The 229 patients with cryptogenic stroke and the 314 control patients were divided into 2 groups according to age (<55 or ≥55 years), and their respective clinical data are listed in Tables 1 and 2 . The prevalence of PFO was significantly higher in younger patients with cryptogenic stroke than in their control group (p = 0.006; Table 1 ). The incidence of atrial septal aneurysm and the prevalence of complex atheroma located in the ascending aorta and aortic arch or the descending aorta in these younger patients were similar in the 2 groups. Multivariate analysis adjusted for age, gender, race, presence of hypertension, diabetes mellitus, hypercholesterolemia, smoking, and coronary artery disease showed that PFO continued to be independently associated with cryptogenic stroke (odds ratio 2.4, 95% confidence interval 1.3 to 4.5, p = 0.007).
| Characteristic | Patients With CS | Patients Without CS | p Value |
|---|---|---|---|
| (n = 114) | (n = 171) | ||
| Age (years) | 42 ± 10 | 42 ± 9.4 | NS |
| Men | 49 (43%) | 72 (42%) | NS |
| Black | 45 (40%) | 53 (31%) | NS |
| White | 63 (55%) | 113 (66%) | NS |
| PFO | 31 (27%) | 24 (14%) | 0.006 |
| Atrial septal aneurysm | 4 (3.5%) | 5 (2.9%) | NS |
| Complex atheromas (located in ascending aorta and arch) | 11 (9.6%) | 12 (7.0%) | NS |
| Complex atheromas (located in descending aorta) | 10 (8.8%) | 13 (7.6%) | NS |
| Hypertension | 58 (51%) | 88 (52%) | NS |
| Diabetes mellitus | 33 (29%) | 42 (25%) | NS |
| Hypercholesterolemia ⁎ | 36 (32%) | 20 (12%) | <0.001 |
| Smokers | 42 (37%) | 72 (42%) | NS |
| Coronary artery disease † | 14 (12%) | 15 (8.8%) | NS |
⁎ Total cholesterol ≥200 mg/dl.
† Significant disease was considered present if there was stenosis ≥70% in an epicardial vessel or 1 of its major branches.
| Characteristic | Patients With CS | Patients Without CS | p Value |
|---|---|---|---|
| (n = 115) | (n = 143) | ||
| Age (years) | 65 ± 8.1 | 66 ± 7.3 | NS |
| Men | 52 (45%) | 71 (50%) | NS |
| Black | 38 (33%) | 67 (47%) | 0.025 |
| White | 75 (65%) | 75 (52%) | 0.039 |
| PFO | 28 (24%) | 21 (15%) | 0.049 |
| Atrial septal aneurysm | 11 (9.6%) | 13 (9.1%) | NS |
| Complex atheromas (located in ascending aorta and arch) | 29 (25%) | 35 (25%) | NS |
| Complex atheromas (located in descending aorta) | 40 (35%) | 43 (30%) | NS |
| Hypertension | 92 (80%) | 107 (75%) | NS |
| Diabetes mellitus | 53 (46%) | 52 (36%) | NS |
| Hypercholesterolemia ⁎ | 33 (29%) | 27 (19%) | NS |
| Smokers | 45 (39%) | 48 (34%) | NS |
| Coronary artery disease † | 21 (18%) | 48 (34%) | 0.005 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


