10 Clinical Trials of Atrial and Ventricular Pacing Modes
 History and Rationale for Different Pacing Modes
History and Rationale for Different Pacing Modes
Cardiac pacing has been developed to treat syncope caused by bradycardia and asystole, initially in patients with permanent third-degree atrioventricular (AV) block. For this purpose, a single lead implanted in the ventricle and pacing at a prespecified rate was sufficient. This simple method of pacing (later coded “VOO 70”) was able to demonstrate a mortality reduction in patients with AV block despite that pacemaker implantation required open-chest surgery at that time.1 Cardiac pacing in permanent third-degree AV block was found not only to prevent syncope, but also to improve symptoms, exercise capacity, and prognosis. It was therefore also used for other patients with bradycardia, such as from intermittent high-degree AV block and sinus node disease (SND).
With technical advancement, the limitations of fixed-rate ventricular pacing were overcome by the development of sensors to provide rate-adaptive (R) ventricular pacing. Rate-adaptive pacing was used to improve the hemodynamic benefit of ventricular single-chamber pacing by providing ventricular rates that take into account the metabolic needs of the patient. In patients with SND, however, ventricular single-chamber pacing in VVI and VVI(R) modes did not reduce mortality2 and could even cause symptoms that were later termed pacemaker syndrome.3 To treat SND, atrial single-chamber pacing has been used, particularly in the Scandinavian countries,4 although many physicians remained skeptical about atrial pacing because it could not prevent asystole if AV block occurred.5 However, a number of advantages of atrial versus ventricular single-chamber pacing were observed, including the absence of pacemaker syndrome, better cardiac output and exercise capacity, resolution of mitral regurgitation that could be induced by ventricular pacing, and a lower incidence of atrial fibrillation.
Comparison Studies
Ventricular Pacing with Versus Without Rate Response (VVI vs. VVIR)
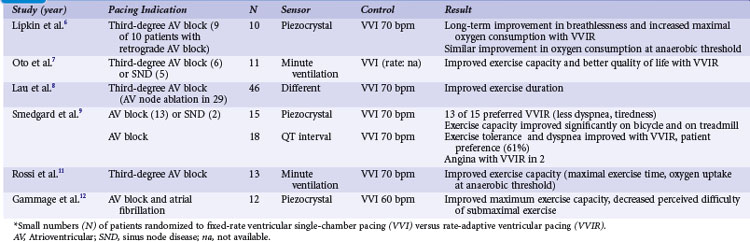
Crossover studies in the 1980s and early 1990s randomized small numbers of patients to fixed-rate ventricular single-chamber pacing (VVI) versus rate-adaptive ventricular pacing (VVIR) with the use of different sensors6–12 (Table 10-1). These studies unequivocally favor rate-adaptive pacing and showed an improvement in submaximal and maximal exercise in terms of objective data (e.g., exercise duration, maximal exercise capacity in watts or duration, VO2 at anaerobic threshold) or subjective data (e.g., pacing mode preference, symptom scores/questionnaires) compared with fixed-rate VVI pacing. This advantage was still present in studies that included patients with SND or retrograde AV conduction. The most striking advantage of VVIR over VVI pacing was observed in patients with AV node ablation for atrial fibrillation.
Ventricular Pacing with Rate Response Versus Dual-Chamber Pacing (VVIR vs. VDD/DDD/DDDR)
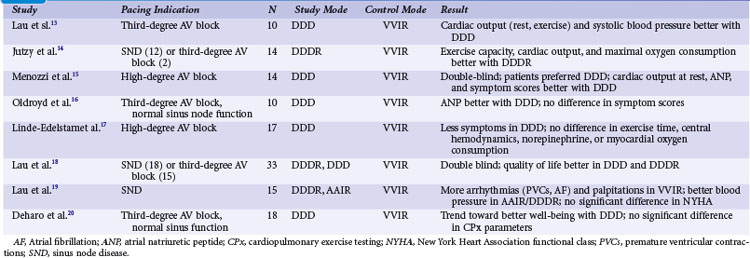
With the advent of dual-chamber pacing, a number of trials tested if rate-adaptive ventricular pacing (VVIR) with an artificial sensor driving the heart rate was comparable to dual-chamber pacing, in which the sinus node determines the heart rate. Investigators observed that sensors frequently reacted inappropriately and were therefore inferior to a chronotropically competent sinus node to increase the heart rate linearly according to metabolic needs during exercise.13 Most studies showed a superiority of dual-chamber pacing in terms of exercise capacity, symptoms, and hemodynamic parameters13–20 (Table 10-2).
Ventricular Single-Chamber Pacing Versus Atrial Synchronized Ventricular Pacing (VVI vs. VDD)
The question if dual-chamber pacing with ventricular pacing synchronized to atrial activity was superior to single-chamber ventricular pacing was evaluated early. In 16 patients with high-degree AV block, Kruse and Rydén21 found a significant increase in maximal exercise capacity in VDD compared to VVI pacing. Interestingly, the extent of improvement was the same for patients older and younger than 65 years. At comparable exercise levels, the atrial rate was significantly lower in VDD than VVI pacing. In a crossover design, 13 patients underwent invasive hemodynamic measurements after 3 months of VDD and VVI pacing.22 During VDD pacing, cardiac output was significantly higher (>30%), particularly during exercise, because of the heart rate increase in VDD and despite a stroke volume increase in VVI pacing. Arteriovenous oxygen difference was significantly higher during VVI pacing. Arterial blood lactate was significantly higher in VVI than VDD pacing during exercise. Heart size was significantly smaller with VDD pacing. In a questionnaire on symptoms and pacemaker choice, patients preferred the VDD mode.
Single-Lead VDD Pacing Versus Dual-Chamber DDD Pacing in Atrioventricular Block
The VDD pacing mode offers the advantage of using only one lead, typically tripolar or quadripolar, with two floating rings that sense atrial activity.23 This pacing mode may be similar to DDD pacing with two leads in patients with AV block and normal sinus node function. However, no RCTs have been performed comparing VDD and DDD pacing. A retrospective study analyzed 1214 consecutive patients with pacemaker implantation for AV block (36.5% VVI; 32.9% DDD; 30.6% VDD).24 At implantation, operation and fluoroscopic times were longer in DDD than in VDD and VVI systems. During follow-up of 5 years, complications requiring surgical interventions occurred 2.3 times more frequently for DDD systems than VDD systems, mainly because of a higher incidence of early atrial lead dysfunction.
Dual-Chamber Pacing in Chronotropic Incompetence or Paroxysmal Atrial Fibrillation: DDD(R) with Mode Switching
Sulke et al.25 compared DDDR, DDD, DDIR, and VVIR pacing modes in 22 patients with high-degree AV block and chronotropic incompetence. In a randomized double-blind crossover design, patients were paced in each of these modes for 4 weeks. Patients were asked their preference, received three questionnaires for subjective assessment, and underwent treadmill testing, mental stress testing, testing of everyday activities (e.g., suitcase lifting, staircase climbing), and echocardiographic evaluation. Scores for subjective grading of well-being were highest for DDDR pacing, similar for DDD and DDIR modes, and lowest for VVIR pacing. DDDR pacing was the preferred mode in 59% of patients, VVIR mode was the least acceptable mode for 73% of patients. Treadmill testing was best in DDDR mode; nontracking modes underresponded to mental stress; and all rate-adaptive modes overreacted to staircase descent. Cardiac output was best in DDDR mode and non-tracking modes showed varying values in patients with AV block. This study suggested that rate-responsive dual-chamber tracking mode is superior to nontracking dual-chamber pacing, dual-chamber pacing without rate-response, and single-chamber ventricular pacing in patients with AV block and chronotropic incompetence, based on both objective and subjective measurements.
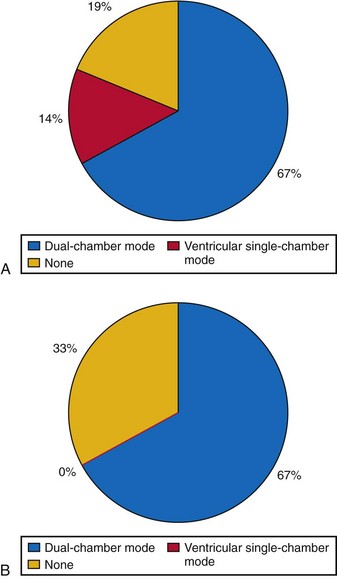
Another study compared different pacing modes in 48 patients with AV block and paroxysmal atrial tachyarrhythmias.26 Patients received dual-chamber systems programmed to DDIR mode for 30 days. In a randomized double-blind crossover manner, devices were then programmed for 4 weeks each to DDDR with mode switching, DDDR with limitation of the upper tracking rate, and VVIR. Patients received transtelephonic self-activated devices to transmit electrocardiograms whenever they perceived symptoms. In addition, at the end of each 4-week study period, devices were interrogated; patients underwent 24-hour Holter recordings, received three symptom questionnaires, and at the end of the study were asked for their preferred pacing period. Patients with intolerable symptoms were allowed to cross over early to the next pacing mode. Different devices with fast- and slow-reacting mode-switching algorithms were used. In this study, one third of patients requested early crossover from VVIR to another mode because of intolerable symptoms, most likely pacemaker syndrome. In DDDR pacing without mode switching but limited upper tracking rate, 19% of patients requested early crossover (29% of patients with documented atrial tachyarrhythmias during this period). Only one patient with DDDR and mode switching requested early crossover because of inappropriate tracking of atrial tachyarrhythmia. Patients with fast-reacting mode-switching algorithms in particular preferred DDDR over VVIR mode. Symptom questionnaires favored DDDR with mode switching over DDDR with limited upper racking rates, DDIR, and VVIR pacing. The authors conclude that dual-chamber pacing with tracking and mode switching to a nontracking mode, whenever this automatic function is fast and reliable, is the preferred pacing mode for patients with AV block and paroxysmal atrial tachyarrhythmias (Fig. 10-1).
Dual-Chamber Pacing with Versus Without Rate Response (DDD vs. DDDR)
The need for a sensor in patients with chronotropic incompetence has received little attention after dual-chamber pacing became available and resolved this problem for patients with AV block and normal sinus function. Most studies subsequently compared different sensors.27,28 Additionally, the definition of “chronotropic incompetence” varied widely.
An early study evaluated cardiopulmonary exercise testing with the DDDR versus DDD pacing modes in eight patients.29 Unfortunately, this was a mix of patients, five with AV block and three with sinus node disease, and five with and three without chronotropic incompetence. Chronotropic incompetence was defined as a maximum heart rate at exercise before pacemaker implantation of less than 110 beats per minute (bpm), but not whether it was caused by AV block (resolved with DDD pacing alone) or sinus node dysfunction (requires rate-adaptive pacing). In a crossover study, patients were randomized to DDD or DDDR, each for 3 weeks, and performed an exercise test and completed a symptom evaluation form at the end of each study period. Rate-adaptive pacing was associated with a higher oxygen uptake at the anaerobic threshold and maximum exercise. However, exercise time and subjective symptoms were not different in the whole patient group, only in patients with chronotropic incompetence, and symptoms of exercise intolerance were better with DDDR pacing.
In a study in 63 patients with a DDD pacemaker, a symptom-limited exercise test was performed 1 month after implantation.30 With chronotropic (sinus node) incompetence defined as a maximum heart rate of less than 60% of the age-predicted maximum or less than 100 bpm, 25 patients were then randomized to perform exercise testing in DDD or DDDR mode on two consecutive days. To minimize bias, patients and physicians were blinded with respect to the pacing mode. Paired analysis revealed a statistically significant improvement in the DDDR mode, with higher heart rates at maximum exercise (113 vs. 84 bpm), longer duration of total exercise and time to anaerobic threshold, and higher oxygen uptake at maximum exercise and anaerobic threshold.
Only one large RCT performed according to the principles of evidence-based medicine (EBM) specifically assessed the benefit of rate-adaptive pacing in the dual-chamber mode in patients with sinus rhythm.31 Unfortunately, the single-blind Advanced Elements of Pacing Randomized Controlled Trial (ADEPT) included a mix of patients with SND (~66%) and AV block. After an exercise test 1 month after implantation, 872 patients were enrolled. To be eligible, patients needed to complete at least stage 2 on the Chronotropic Assessment Exercise Protocol and to have a heart rate at peak exercise of 80% or greater of the age-predicted maximum. The mean age was 71 years, however, so patients with a maximum heart rate not exceeding 120 bpm at maximum exercise could be included. Patients were randomized to DDD versus DDDR pacing (dual-sensor system; maximum adaptive rate, 220 bpm minus age) with rate-adaptive AV delay shortening in a parallel study design. After 12 months, general QOL (measured by Short-Form 36 General Health Survey [SF-36], Ferrans and Powers Quality of Life Index) and cardiovascular functional status (Specific Activity Scale and Duke Activity Status Index) were assessed by questionnaires, together with the maximum exercise time at treadmill testing 6 months after randomization. ADEPT found no specific or general differences in scores of the activity and QOL questionnaires. The total exercise time was not different between DDD and DDDR pacing. Independent of discussions about the ideal sensor(s), severe limitations included the following:
 Atrial Versus Ventricular Single-Chamber Pacing in Sinus Node Disease
Atrial Versus Ventricular Single-Chamber Pacing in Sinus Node Disease
In 1994, Andersen et al.34 published the first RCT on pacing mode. A total of 225 patients with SND were randomized to receive a single-chamber pacemaker in the right atrium or ventricle. Of note, the study excluded patients with AV block of any degree (including first-degree AV block with PQ interval >220/260 msec), Wenckebach block at less than 100 bpm, atrial fibrillation (AF) more than 50% of the time (or with pauses >3 seconds or ventricular rates <40 bpm), or bifascicular bundle branch block. In total, 827 of 1052 screened patients were excluded from study participation, predominantly because of AV block (n = 552). Study outcome parameters were mortality, AF, thromboembolism (TE), and heart failure (HF). From retrospective studies, the authors expected AF in 30%, TE in 15%, and mortality in 15% of patients in the ventricular pacing group. The study intent was to demonstrate a 50% reduction in AF and HF and a 66% reduction in TE and mortality with atrial single-chamber pacing, which would have required 100 patients in each group. This rather optimistic prediction of the capabilities of physiologic pacing reflects the widespread belief in its superiority over ventricular pacing at the time of conception of this study.
Andersen et al.35 extended the follow-up until the last patient completed 5 years in the assigned pacing mode. By that time, the first patients enrolled into the trial had completed an 8-year follow-up (mean, 5.5 years). This prolonged follow-up demonstrated a significantly lower mortality in atrial versus ventricular pacing (relative risk reduction [RRR], 34%), mainly from a reduction in cardiovascular mortality (Table 10-3). Similarly, atrial fibrillation was less likely in the atrial pacing group (RRR, 46% vs. ventricular pacing) as were TE events (RRR, 53%). Only 4 of 110 patients developed AV block during the study period (annual rate, 0.6%), two of whom had a right bundle branch block at baseline. The authors detected retrograde conduction in 63% of patients randomized to VVI pacing.
TABLE 10-3 Clinical Events in Atrial versus Ventricular Pacing for Sick Sinus Syndrome (Danish Study)*
| Clinical Event | Ventricular (n = 115) | Atrial (n = 110) |
|---|---|---|
| All-cause mortality | 50% | 34%† |
| Cardiovascular mortality | 34% | 17%† |
| Stroke (cerebrovascular accident) | 23% | 12%† |
| NYHA functional class | Mean 1.3 | Mean 1.5† |
| Permanent atrial fibrillation | 8% | 19%† |
* Results from long-term follow-up.
† P < .05 for lower incidence respectively; better value with AAIR.
From Andersen HR, Nielsen JC, Thomsen PE, et al: Long-term follow-up of patients from a randomised trial of atrial versus ventricular pacing for sick-sinus syndrome. Lancet 350:1210-1216, 1997.
Critical Appraisal of Danish Study
The Danish study34,35 was the first large-scale RCT on pacing mode selection, at a time when the discussion was whether it was ethically possible to implant VVI(R) pacemaker systems in SND patients. Also, it is as yet the most positive RCT in favor of atrial-based pacing. Compared with RCTs on dual- versus single-chamber ventricular pacing, however, the number of patients in the Danish trial was rather small; the expectations of a 50% AF and HF reduction and even 66% TE and mortality reduction by atrial versus ventricular single-chamber pacing were too optimistic to show a significant difference in such a small patient group. Prolongation of follow-up to cope with this error in sample size calculation was not prespecified, thus arguably not allowed in a prospective trial. Therefore, results resemble a “post hoc” analysis and are only hypothesis generating. However, all results at 3.3 and 5.5 years point to atrial pacing being associated with more favorable clinical results than ventricular pacing. In no study outcome parameter was ventricular better (significantly or nonsignificantly) than atrial pacing.
The Danish trial proposed effective criteria to select patients for AAIR pacing with low risk of AV block. The need to measure the Wenckebach block point at study entry in addition to the PQ interval, however, is not clear. During the study, no development of AV block was predictable by a progressive reduction in the heart rate at the Wenckebach block point.36 However, only a few patients who had documented second-degree or third-degree AV block received an upgrade from AAI to DDD. An observational study found an annual incidence of upgrade from AAI to DDD of 1.7% as a result of documented AV block or AF with slow ventricular rate in 399 patients followed for 4.6 years.37 Also of note was a 0.8% additional annual reoperation rate for the addition of a ventricular lead, mainly because of atrial lead problems. Therefore, 2.5% of AAI systems were surgically changed to VVIR or DDDR per year.
There is renewed interest in the Andersen et al.34,35 data because of the deleterious effects of unnecessary right ventricular pacing observed in the DDDR mode38 (see later). In this context, observations from the Danish trial on development of heart failure with VVI pacing in sinus node disease are important.39 The Danish trial observed an increase in New York Heart Association (NYHA) functional class during follow-up in 31% of patients in the ventricular versus 9% in the atrial group (P < .0005). The incidence of crural edema and dyspnea, together with the need for diuretics during the 5.5-year study period, was significantly higher in patients with ventricular pacing, and the left ventricular fractional shortening decreased significantly only in the ventricular group, not in the atrial pacing group. At the same time, the left atrial diameter increased significantly more during ventricular pacing, from 34 to 41 mm. Interestingly, despite the left atrial dilatation in ventricular pacing in SND, a higher incidence of AF was evident only after 5.5 years, not at 3.3 years of follow-up, despite that TE events were observed more frequently in ventricular pacing already at 3.3 years. Of note, 12 of the 39 patients who developed TE during follow-up never had documentation of AF, neither before randomization nor during follow-up.40 Documentation may have missed AF in a significant number of patients because only 12-lead ECG was used at follow-up. Pacemaker memory functions likely would have documented a much higher incidence of AF.41
 Ventricular Versus Dual-Chamber Pacing
Ventricular Versus Dual-Chamber Pacing
Nonrandomized Early Studies
Starting from impressive observations of improved hemodynamics with VAT and VDD compared to VVI pacing in patients with AV block,22 many publications documented the benefits of “physiologic” versus ventricular pacing from the earlier 1980s to the late 1990s. Various parameters were used to define the presence or absence of this benefit (Table 10-4). Outcomes of dual-chamber or atrial versus ventricular single-chamber pacing particularly note hemodynamic improvement with dual-chamber pacing and range from case reports to patient series.42 Of these multiple outcome parameters, four were frequently chosen as endpoints in prospective, large-scale RCTs: mortality, stroke, atrial fibrillation, and heart failure. Whereas studies of the early 1980s usually focused on hemodynamic parameters, the concept of clinical studies on pacing shifted toward investigating the impact of different pacing modes on clinical events such as mortality, particularly after the CAST study, in which antiarrhythmic drugs successfully suppressed ventricular ectopy but were associated with an increased mortality.
TABLE 10-4 Evaluation Parameters for Impact of Pacing Modes on Cardiac Performance
| Area | Parameters |
|---|---|
| Clinical | |
| Exercise capacity | |
| Echocardiographic | |
| Clinical events | |
| Invasive hemodynamics | |
| Blood serum | |
| Coronary artery perfusion | |
| Arrhythmias |
LV, Left ventricular; NYHA, New York Heart Association.
Mortality
Retrospective early trials showed a significant reduction of mortality for atrial and dual-chamber pacing compared to ventricular single-chamber pacing, predominantly in patients with sinus node disease43–52 (Tables 10-5 and 10-6). However, mortality rates varied widely for VVI (15%-48%) compared to atrial or dual-chamber pacing (7%-27%).50
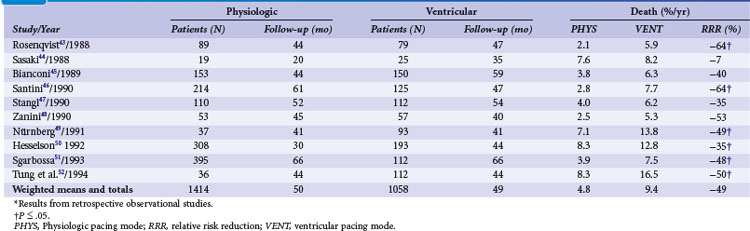
TABLE 10-6 Survival in Patients with Atrioventricular Block and Other Indications in Relation to Pacing Mode*

In high-degree AV block, Alpert et al.53 found no difference in all-cause mortality between 132 patients with ventricular compared to 48 patients with dual-chamber systems. Similarly, in 148 patients with AV block (74 with VVI and 74 with VDD pacemaker systems), Linde-Edelstam et al.54 found no difference in mortality in the entire patient group. However, both studies found that in patients with preexisting heart failure, VVI pacing was associated with a significantly higher mortality than VDD pacing. A study of 1245 patients (77% with AV block; ventricular pacing in 97%, dual-chamber pacing in only 3%), suggested that survival was related to the mode of pacing.48 Analyzing 391 patients with AV block or carotid sinus hypersensitivity, Hesselson et al.50 demonstrated a significant mortality benefit during a 7 year follow-up with DDD (54%) versus VVI pacing (33%).
Atrial Fibrillation and Thromboembolism
Starting in the 1980s, almost all retrospective studies showed a lower incidence of AF in patients with atrial/dual-chamber pacing compared to ventricular single-chamber pacing43–52,54–59 (Table 10-7). This was particularly evident for SND.
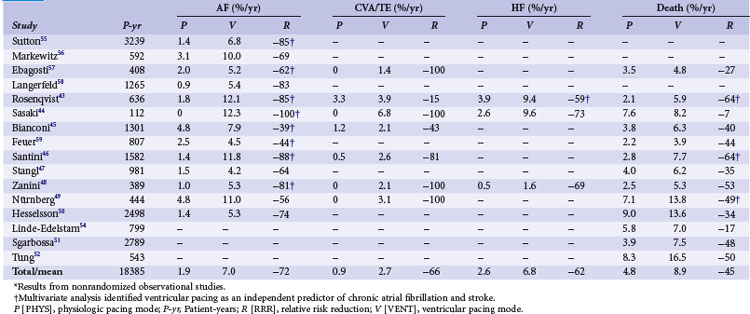
Heart Failure
Several studies identified ventricular versus “physiologic” pacing mode as an independent predictor of mortality in patients with congestive heart failure (CHF),54 whereas others did not confirm this observation.51 Overall, retrospective studies suggest a large improvement in clinical outcomes with the use of atrial and dual-chamber pacing versus ventricular pacing systems, with a 45% RRR in mortality, 62% reduction in HF, 66% reduction in stroke, and a 72% reduction in AF (see Table 10-7). These data were used to calculate sample size in the Danish trial of AAI versus VVI pacing.34
Medicare Trial
As with other investigators in the late 1980s, Lamas60 noted the problem of “retrograde,” or ventriculoatrial (VA) conduction during VVI pacing at Brigham and Women’s Hospital (Boston). This was a common phenomenon in pacemaker patients and a significant cause of adverse symptoms after VVI pacemaker implantation. Also, only a properly timed atrial systole contributed positively to systolic ventricular performance by the Frank-Starling mechanism which states that the extent of systolic myocardial fiber shortening depends on the degree of diastolic fiber stretch, or preload. Therefore, with the important atrial contribution to cardiac performance, dual-chamber pacing with restoration of normal cardiac physiology (AV synchrony and appropriate rate response) may be advantageous in patients with AV block or SND.
Lamas et al.61 sought to confirm the theoretical advantages of dual-chamber pacing in a large, retrospective analysis of a 20% random sample of all Medicare beneficiaries 65 or older who received a first pacemaker implantation (1988-1990) and whose vital status information was available for at least 1 year (n = 36,312). Dual-chamber pacemaker selection was an independent predictor of survival at 1 and 2 years, with a relative mortality risk reduction of 18%, even after controlling for potentially confounding factors. However, choice of dual- versus single-chamber pacing mode was biased by patient age, gender, indication for pacing, presence of CHF, and AF. Additionally, implantation in the western United States, rural provider, and hospitalization in a facility with 500 beds or more, a private hospital, or a hospital with a catheterization laboratory were also associated with dual- instead of single-chamber pacemaker selection. For this potential bias, the authors performed a prospective trial.
Randomized Studies
In the early 1980s, double-blind crossover studies prospectively compared VVI to dual-chamber pacing. Perrins et al.62 randomized 13 patients with AV block and a VDD pacemaker to dual-chamber or VVI mode. They found a better exercise capacity and reduction of symptoms during the period with dual-chamber pacing, as documented by patients’ diaries and monthly symptom scores. Similarly, Kristensson et al.63 randomized 44 patients to VVI or VDD for 3 weeks for each mode. They observed a statistically significant improvement of maximal exercise tolerance of 14% with AV synchronous pacing. Arterial lactate, respiratory rates, and perceived exertion ratings during submaximal exercise were higher on ventricular inhibited pacing. Symptom scores during the 3-week periods with VVI pacing were worse than with dual-chamber pacing. Most patients had a better functional class during AV synchronous pacing and preferred this pacing mode.
In one of the first prospective randomized, intention-to-treat trials on pacing mode selection, Mattioli et al.64 compared ventricular (VVI or VVIR) with physiologic pacing (AAI, DDD, DDDR, VDD) in 210 patients (SND in 110, AV block in 100) with a median age of 77 years. Only six patients received an AAI pacemaker. Patients with previously known AF were excluded from this study. A total of 56 patients (27%) developed AF during follow-up. The incidence of AF was 10% at 1 year, 23% at 3 years, and 31% at 5 years. The investigators observed an increased incidence of chronic AF in patients receiving ventricular pacing (P < .05). No difference was observed in the incidence of chronic AF between patients paced for AV block and patients paced for SND. In the subgroup of SND patients, the incidence of chronic AF was significantly less in patients receiving a physiologic than in those receiving a ventricular pacemaker (see Table 10-7).
Pacemaker Selection in the Elderly Study (PASE)
After their observations in the Medicare trial, Lamas et al.65 randomized 407 patients 65 or older with sinus rhythm and an indication for permanent pacing (SND or AV block) to single- or dual-chamber pacemaker therapy in the Pacemaker Selection in the Elderly Study. All patients received a dual-chamber device programmed to VVIR or DDDR according to the randomization result. The primary endpoint was health-related QOL (measured by SF-36); average age was 76. During the 30-month follow-up, QOL improved significantly after pacemaker implantation, but without a significant difference between VVIR and DDDR pacing modes, neither in QOL nor in clinical outcomes (cardiovascular events or death; Table 10-8). However, this refers to the intention-to-treat analysis while “on-treatment”, 26% percent of patients assigned to ventricular pacing were crossed over and paced in the dual-chamber mode because of symptoms of pacemaker syndrome.
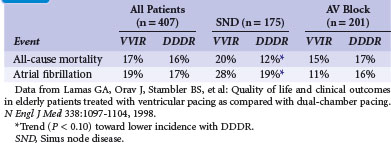
The PASE subgroup of patients with SND had a significantly better QOL in some subscales of the SF-36 and a better cardiovascular functional status with dual-chamber pacing than with ventricular pacing. A trend toward lower all-cause mortality, lower incidence of AF, and reduced incidence of the combined endpoint of stroke, hospitalization for heart failure, or all-cause mortality favoring dual-chamber pacing was seen in patients with SND, but not in those with AV block (see Table 10-8). The authors concluded that pacemaker therapy improves QOL, but that the benefits associated with dual-chamber pacing versus ventricular pacing were moderate and observed only in the subgroup of SND patients.
Critical Appraisal
PASE was the first large multicenter RCT on dual-chamber versus ventricular single-chamber pacing performed according to EBM guidelines. The results were primarily interpreted as disappointing, showing only a marginal or even no advantage of dual-chamber pacing. However, the most relevant clinical finding may be the crossover rate of 26% from VVIR to DDDR pacing because of symptoms potentially caused or worsened by single-chamber pacing. In PASE, all patients had received dual-chamber devices, and randomization to single- or dual-chamber pacing was performed by device programming (“software randomization”). Patients randomized to VVIR pacing thus were fortunate because crossover did not require an additional surgical intervention, only reprogramming. Therefore, it was argued that crossover may have been performed because of bias on the side of physicians who attributed symptoms during VVIR pacing inappropriately to “pacemaker syndrome,” despite that per protocol, investigators were required to discuss each case individually with the principal investigator. An analysis of causes and results of crossover from VVIR to DDDR pacing, however, showed that the most common reason for crossover was “severe pacemaker syndrome” (77%), defined as a constellation of fatigue, dyspnea, effort intolerance, paroxysmal nocturnal dyspnea, neck fullness, presyncope, cannon A waves, blood pressure (BP) reduction with ventricular pacing, and CHF initiation or exacerbation.66 The most common individual symptoms were fatigue (62%), effort intolerance (64%), dyspnea (55%), and presyncope (34%). The diagnosis “pacemaker syndrome” or “intolerance to VVIR” in these patients with crossover is supported by the observation that, in contrast to other patients, their QOL deteriorated significantly after pacemaker implantation before crossover and improved significantly after reprogramming to dual-chamber pacing. The use of β-blockers, the presence of nonischemic cardiomyopathy, and systolic BP less than 110 mm Hg during ventricular pacing (relative risk of crossing over = 2.6) predicted intolerance to VVIR. However, the sensitivity of a decrease in paced systolic BP to less than 110 mm Hg at implantation for predicting intolerance to VVIR pacing was only 36%, the positive predictive power only 48%. The presence of VA conduction at implant did not predict the development of intolerance to VVIR pacing, although VA conduction or cannon A waves were present in almost 50% of crossover patients.
Mode Selection Trial in Sinus Node Dysfunction (MOST)
The group of investigators of PASE followed their observation that differences in outcome parameters between VVIR and DDDR were (if present at all) more pronounced in sinus node disease, performing a pacing mode comparison in SND patients.67 A total of 2010 patients were randomized to dual-chamber (1014) or ventricular pacing (996) and followed for 33 months. The incidence of the primary endpoint (all-cause mortality or nonfatal stroke) did not differ significantly (21.5% in DDDR, 23.0% in VVIR). Adjusted analyses revealed that in patients assigned to DDDR pacing, the risk of AF was 23% lower (21% vs. 27%) and HF scores were better. Heart failure hospitalization was reduced by 27%, the composite endpoint death, stroke, or HF hospitalization was reduced by 15% (Table 10-9). Dual-chamber pacing resulted in significantly better QOL for six of the eight SF-36 subscales during the 4 years of follow-up. The authors concluded that in SND patients, dual-chamber pacing does not increase stroke-free survival compared to ventricular single-chamber pacing, but DDDR significantly reduces AF risk and HF symptoms and improves QOL.
TABLE 10-9 Clinical Events in Mode Selection Trial in Sinus Node Dysfunction (MOST)
| Clinical Event | VVIR (n = 996) | DDDR (n = 1014) |
|---|---|---|
| Death | 23.0% | 21.5% |
| Stroke | 4.9% | 4.0% |
| Heart failure hospitalization | 12.3% | 10.2%* |
| Atrial fibrillation | 27.1% | 21.4%* |
* P < .05 for lower incidence with DDDR.
Data from Lamas GA, Lee KL, Sweeney MO, et al: Ventricular pacing or dual-chamber pacing for sinus-node dysfunction. N Engl J Med 346:1854-1862, 2002.
Critical Appraisal
The MOST trial had the ambitious aim to assess clinical events (mortality, stroke), AF incidence, and symptoms (HF, pacemaker syndrome, QOL) in VVIR versus DDDR pacing for SND. While the latter two endpoints favored dual-chamber pacing, the first and most important endpoint (mortality) did not demonstrate a significant difference. Therefore, the MOST trial was frequently regarded as a negative trial, showing no significant benefit of dual-chamber compared to ventricular single-chamber pacing. In-depth analyses of mortality68 and stroke risk69 showed no advantage of dual-chamber pacing, and QOL was better in dual-chamber mode in several items, particularly related to physical function.70 However, there were two important lessons from MOST: (1) pacemaker syndrome is frequent in SND and VVIR pacing,71 and (2) unnecessary right ventricular pacing in SND is detrimental.38
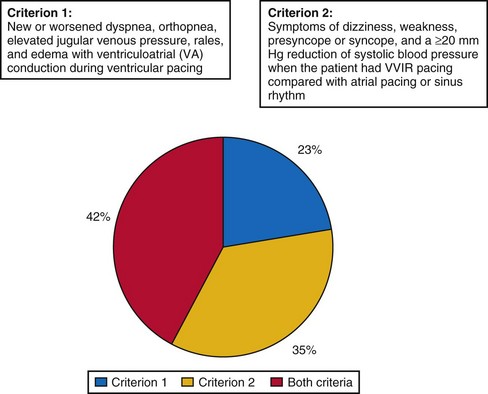
A strong argument in favor of dual-chamber pacing is the observation of severe pacemaker syndrome in approximately 20% of SND patients treated by VVIR pacing.71 The investigators in MOST attempted to prevent the major weakness of PASE, where the crossover rate from single- to dual-chamber pacing of 26% was so high that it may have prevented any meaningful intention-to-treat analysis of the difference between the two pacing modes. In MOST, therefore, the diagnosis of pacemaker syndrome strictly required documentation of new symptoms (e.g., dyspnea, syncope) together with VA conduction or systolic BP reduction of 20 mm Hg or more during VVI pacing compared to intrinsic rhythm. Even in the presence of pacemaker syndrome, crossover of pacing mode had to be confirmed by the clinical coordinating center; other attempts to resolve pacemaker syndrome (e.g., reprogram pacing rate, deactivate sensor) were required; and only if these failed, the centers could ask the principal investigator to review the indication for crossover to dual-chamber mode.
Despite these rigid requirements, 20% of patients programmed to VVIR met criteria for pacemaker syndrome and required crossover from single- to dual-chamber. Interestingly, pacemaker syndrome could basically develop at any time after implantation: At 6 months, it was present and required reprogramming in 14% of patients with VVIR pacing, in 16% at 1 year, in 18% at 2 years, and in 20% at 4 years. Slow sinus rates but not the presence or absence of VA conduction before pacemaker implantation predicted the development of pacemaker syndrome. QOL in patients with pacemaker syndrome was significantly worse than in patients without this complication of VVIR pacing, and it improved significantly after crossover to dual-chamber mode. Therefore, pacemaker syndrome with 20% incidence can be regarded as the most frequent complication of ventricular single-chamber pacing in SND, with significant impact on patients’ symptoms and QOL (Fig. 10-2).
A second post hoc analysis of MOST detected one of the basic problems of studies on mode selection and changed the practice of cardiac pacing. Sweeney et al.38 found that the percentage of right ventricular (RV) pacing was strongly associated with the risk of developing HF and AF. This refers to patients with SND and narrow QRS at baseline. Interestingly, this association was more striking for dual-chamber than single-chamber pacing. From these results, hypothetically, a “badly timed” (i.e., too early) ventricular stimulus may be more detrimental in dual-chamber pacing, where the pacing mode forces adverse AV timing to be present in every cycle, versus single-chamber ventricular pacing, where (besides pacemaker syndrome with VA conduction) only some cycles have by chance a detrimental AV relation, whereas in most cardiac cycles, atrium and ventricle are dissociated.
Canadian Trial of Physiologic Pacing (CTOPP)
After PASE in 1998, the Canadian Trial of Physiologic Pacing was the second large RCT on pacing mode selection.72 It enrolled patients scheduled for pacemaker implantation without permanent atrial fibrillation at 32 Canadian centers. Patients were randomized to receive either a ventricular pacemaker or a “physiologic pacemaker” (i.e., atrial single or dual chamber) and followed for an average of 3 years. The primary outcome was stroke or death from a cardiovascular cause; secondary outcomes were all-cause mortality, AF development, and hospitalization for heart failure. CTOPP randomized 2568 patients, 1094 received a physiologic system (dual-chamber or atrial single-chamber pacemaker), and 1474 a ventricular single-chamber device. The annual rate of stroke and death from cardiovascular causes were similar in both groups (5.5% with ventricular pacing, 4.9% with physiologic pacing; P = 0.33) (Table 10-10). The incidence of AF was lower with physiologic versus ventricular pacing (annual rate, 5.3% vs. 6.6%; P = .05) with the difference emerging only 2 years after implantation. All-cause mortality and HF hospitalization were not significantly different, whereas postoperative complications occurred more frequently with physiologic pacing (9.0%), which consisted of atrial single-chamber pacing in only 5% and ventricular single-chamber pacing in another 5% of patients because of problems to implant the atrial lead. The authors of CTOPP concluded that physiologic pacing provides little or no benefit over ventricular pacing with regard to stroke prevention or cardiovascular death.
TABLE 10-10 Clinical Events in Canadian Trial of Physiologic Pacing (CTOPP)
| Clinical Event (annual) | VVIR (n = 1474) | AAIR/DDDR (n = 1094) |
|---|---|---|
| Stroke | 1.1% | 1.0% |
| Heart failure hospitalization | 3.5% | 3.1% |
| Atrial fibrillation | 6.6% | 5.3%* |
* P ≤ .05 for lower incidence with DDDR.
Data from Connolly SJ, Kerr CR, Gent M, et al: Effects of physiologic pacing versus ventricular pacing on the risk of stroke and death due to cardiovascular causes. N Engl J Med 342:1385-1391, 2000.
Critical Appraisal
A post hoc analysis supported the criticism that the lack of benefit of physiologic pacing may derive from CTOPP including many patients with only intermittent and rare bradycardia. Tang et al.73
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


