Chest Wall Tumors
Bernard J. Park
Raja M. Flores
Chest wall tumors arise from a wide variety of benign and malignant etiologies and confront the clinician with a diagnostic and therapeutic challenge. More than half are malignant, and most of these are the result of metastases or direct invasion from adjacent tumors of the thorax, mediastinum, or soft tissue. Primary chest wall tumors are rare; of these, soft tissue tumors account for roughly 50%. Wide surgical resection is the most effective treatment for the vast majority of chest wall tumors. Improvements in reconstructive techniques and care of the perioperative patient have led to low morbidity and mortality rates for chest wall resection. Keys to successful management include accurate diagnosis, wide surgical resection, and appropriate reconstruction of large chest wall defects. The optimal treatment of locally recurrent breast cancer and metastatic lesions to the chest wall is controversial.
Incidence and Location
The majority of chest wall lesions are the result of invasion from adjacent malignancies or metastatic lesions (Table 49-1). There are only a few large surgical series of chest wall lesions that have been characterized following resection.25,27,31,43,46 The largest institutional experience comes from the authors’ institution, Memorial Sloan-Kettering Cancer Center (MSKCC). Martini and coauthors25 reported an initial 20-year experience of 317 consecutive patients undergoing chest wall resection for malignant tumors. Primary lung and breast cancer made up 163 cases (51%), while 71 patients (22%) had metastatic lesions. The recent MSKCC experience summarized by Weyant and colleagues43 described an additional 262 patients who underwent resection for a variety of indications.46 Once again, malignant lesions dominated, with the most common indications being lung cancer (n = 99, 38%), sarcoma (n = 75, 29%), and breast carcinoma (n = 26, 10%). Similarly, in the Emory University experience of 200 chest wall resections, 75 patients (38%) had lung cancer while 53 (27%) had sarcoma and 43 (22%) had breast cancer.27 In most series, sarcomas were the most frequent metastatic tumors.
Primary chest wall tumors, by comparison, are relatively uncommon, representing roughly 5% of all thoracic neoplasms and 1% to 2% of all primary tumors.22 In the Emory experience, only 27% of all chest wall resections were for primary chest wall tumors; 83 (26%) of the 317 chest wall lesions in the early MSKCC experience were primary tumors.25,27 In the Mayo Clinic series of 100 consecutive patients undergoing chest wall resection, 44% of all tumors were primary neoplasms.31
Benign tumors account for approximately half of all primary chest wall neoplasms, with rates ranging from 21% to 67%.3,17,20,23 The most frequently encountered benign lesions are osteochondroma, chondroma, and fibrous dysplasia. Like benign neoplasms, primary malignant tumors generally arise from the soft tissue or the bony and cartilaginous elements of the chest wall. In the MSKCC series, soft tissue sarcomas made up 45% of all primary malignant lesions.7 Desmoid tumor, liposarcoma, and rhabdomyosarcoma are the most frequent histologies of sarcoma encountered. Chondrosarcoma, Ewing’s sarcoma, and osteosarcoma are the most common malignant bone lesions and the most common primary malignant chest wall tumors overall in our experience.
Chest wall neoplasms, primary and metastatic, can arise from or involve any portion of the thoracic skeleton, including the ribs, sternum, scapulae, and clavicles. The most common site of involvement for all chest wall lesions is the rib cage. Primary lesions of the sternum, scapulae, and clavicles are uncommon, but nearly all are malignant.10 Malignant primary chest wall neoplasms can also originate in a previously irradiated field, although this is a relatively uncommon event. Schwarz and Burt37 showed that 6% of patients (21 of 351) with primary chest wall malignancies had received prior irradiation. There is no predominant histologic cell type, with the usual spectrum of lesions occurring.
Diagnosis and Evaluation
Symptoms and Signs
Soft tissue chest wall tumors are generally asymptomatic, initially, presenting as slowly enlarging masses. As Gordon and colleagues16 reported, 73% of patients with primary soft tissue sarcomas of the chest wall presented with a nonpainful mass. With continued growth and tumor involvement of surrounding tissue, pain invariably occurs. The pain is frequently generalized, and the patient commonly is treated for musculoskeletal or neuropathic etiologies. Almost all malignant lesions are likely to become painful, whereas only two-thirds of benign tumors produce pain. Cartilaginous and bony tumors more frequently have pain as one of the first symptoms of disease. Burt7 showed that pain with or without a mass was present in 49% of patients with
chondrosarcoma, in 95% with Ewing’s sarcoma, and in 78% with osteosarcoma. In some cases with rib lesions, a radiographic abnormality can be discovered with no mass palpable on physical examination. Occasionally, there may be systemic manifestations, such as fever, leukocytosis, and eosinophilia.
chondrosarcoma, in 95% with Ewing’s sarcoma, and in 78% with osteosarcoma. In some cases with rib lesions, a radiographic abnormality can be discovered with no mass palpable on physical examination. Occasionally, there may be systemic manifestations, such as fever, leukocytosis, and eosinophilia.
Table 49-1 Series of Chest Wall Resections | ||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Diagnosis
The initial evaluation of any patient suspected of having a chest wall neoplasm begins with a complete history and physical examination. The clinician should pay particular attention to any history of prior malignancy, exposure to ionizing radiation, or presence of familial conditions, such as Gardner’s syndrome or von Recklinghausen’s disease. Standard conventional plain chest radiographs should be obtained and compared with any previous studies if available. Computed tomography (CT) of the chest is the single best radiographic modality to localize and characterize most chest wall tumors in order to generate a differential diagnosis and treatment strategy. In some instances, magnetic resonance imaging (MRI) of the chest can add additional useful information. Compared with CT, MRI can delineate better the extent of muscular invasion, relationship to nearby blood vessels, and/or spinal involvement by chest wall lesions.13,47 CT, however, is superior in the assessment of calcifications and presence of pulmonary pathology. While specific tumors may have features better elucidated by one or the other modality, it is clear that these techniques are complementary. Moreover, while judicious use of imaging and careful analysis of films can often lead to a correct diagnosis, radiographs tend to be most useful in the planning of tissue biopsy or surgical resection.36
Following history, physical examination, and imaging, if there is doubt whether a chest wall neoplasm is benign or malignant or if the lesion is suspected of being a primary tumor, tissue diagnosis by histologic examination is required. Biopsy should be well planned, minimally traumatic to the primary tumor and surrounding tissue, and diagnostic. There are three options: needle biopsy, excisional biopsy, and incisional biopsy.
Needle Biopsy
The benefits of needle biopsy include minimal soft tissue injury, ease of performance, and low complication rate in an outpatient setting. Fine-needle aspiration alone is best employed in patients who are suspected of having a metastasis from a prior documented malignancy. It is not as good for situations such as a primary bony or cartilaginous chest wall tumor, where a larger amount of tissue is required for pathologic diagnosis. Percutaneous core needle biopsy is a viable option for the diagnosis of primary chest wall tumors and is a well-accepted technique for biopsy of primary bone tumors. Welker and coauthors45 demonstrated a diagnostic rate of 92.6% in 161 musculoskeletal tissue masses suspected of being sarcoma.
Excisional Biopsy
Excisional biopsy with minimal margins (1 cm) should be employed for small (<5 cm) primary neoplasms. Closure of the chest wall usually can be performed primarily without reconstruction. If the lesion is benign or best treated with non-surgical-therapy (chemotherapy, radiation, or both), no further operation is required. If the lesion is a primary malignant neoplasm, the patient should undergo reoperation with radical excision with wide margins and appropriate reconstruction.
Incisional Biopsy
Incisional biopsy should be performed when a needle biopsy is nondiagnostic or for primary lesions >5 cm. It is important to orient the skin incision to facilitate its excision at the time of definitive resection and to promote optimal wound healing, avoiding ulceration and infection that might delay therapy. Skin flaps should not be raised, and the deep plane of the tumor, in particular the pleural space, should be left intact to prevent dissemination of tumor cells.
Evaluation
While advances in surgical technique, anesthesia, and perioperative management have reduced morbidity and mortality, extensive chest wall resection and reconstruction remains a major surgical procedure. As with any other thoracic operation, careful preoperative assessment is critical to minimize the risks to the individual patient. In addition to a detailed history and physical examination, this evaluation should include a thorough investigation of cardiopulmonary comorbidities, smoking history, performance status, and psychosocial support. The presence of cardiovascular disease, such as coronary artery or valvular disease, has important implications for intraoperative and postoperative hemodynamic monitoring and fluid management. The authors are in the practice of routinely obtaining cardiac stress testing in patients over the age of 70, in particular if they have a long history of smoking, hypertension, diabetes mellitus, or other manifestations of atherosclerotic disease (peripheral vascular disease, carotid stenosis, aneurysm). If the patient’s pulmonary reserve is of concern, it should be assessed with pulmonary function tests that include spirometry, diffusion capacity, and arterial blood gas analysis. Patients with chronic obstructive pulmonary disease or other active pulmonary disease should have optimal medical treatment prior to surgery.
Preoperative consultation with a variety of subspecialists is often necessary. For instance, in the case of the “medical malignancies,”
such as Ewing’s sarcoma and plasmacytoma, evaluation by medical and radiation oncologists prior to operation is an integral part of their multimodality treatment. Depending on the size of the lesion, chest wall reconstruction may warrant the use of myocutaneous flaps; these procedures are best performed in conjunction with plastic and reconstructive surgeons. Similarly, neurosurgical consultation is often required for tumors encroaching on the spine.29 When complete resection is limited by proximity of the lesion to vital structures, external beam radiotherapy, either preoperatively or postoperatively, or intraoperative brachytherapy should be considered.42
such as Ewing’s sarcoma and plasmacytoma, evaluation by medical and radiation oncologists prior to operation is an integral part of their multimodality treatment. Depending on the size of the lesion, chest wall reconstruction may warrant the use of myocutaneous flaps; these procedures are best performed in conjunction with plastic and reconstructive surgeons. Similarly, neurosurgical consultation is often required for tumors encroaching on the spine.29 When complete resection is limited by proximity of the lesion to vital structures, external beam radiotherapy, either preoperatively or postoperatively, or intraoperative brachytherapy should be considered.42
Surgical Management
In suitable patients, surgical resection for cure is appropriate for primary chest wall neoplasms. In select cases of metastatic lesions and locally recurrent breast cancer, surgical extirpation of an isolated chest wall lesion can result in long-term survival benefit. Even in instances where the likelihood of cure is low, chest wall resection may be indicated to palliate lesions that are unresponsive to nonsurgical therapies (chemotherapy, radiation) and are causing local complications, such as wound ulceration, infection, or intractable pain.
The margin of excision during definitive resection for chest wall lesions varies somewhat depending on the type of neoplasm. Moreover, what constitutes an adequate margin of excision to minimize the incidence of recurrence and maximize chances for long-term survival for patients with a primary malignant chest wall tumor is a matter of some debate. What is clear is that the extent of resection should not be limited to the size of the resulting defect. With a wide variety of techniques available, bony and soft tissue deficits of almost any size can be reconstructed with excellent results.
The technical details of resection and reconstruction are reviewed elsewhere in this textbook and are not covered extensively in this chapter. (See chapter 50.)
Specific Tumors
Primary Bone Tumors
Primary bone neoplasms of the chest wall are uncommon. Dahlin and Unni10 summarized a series of 6,034 bone tumors, of which 355 (5.9%) occurred in either the ribs (85%) or the sternum (15%). Nearly all were malignant (89%), with sternal tumors slightly more likely to be malignant than rib tumors (96% versus 88%). The most common benign bone lesions are osteochondromas, chondromas, and fibrous dysplasia. Martini and coworkers25 reported that fibrous dysplasia accounts for 30% of benign tumors of the chest wall. The most common primary malignant bone tumors seen at MSKCC are chondrosarcoma, Ewing’s sarcoma, and osteosarcoma.7
Benign Rib Lesions
Osteochondroma
While osteochondroma is overall an uncommon tumor, it is the most common benign bone neoplasm, constituting nearly 50% of all benign rib tumors. It arises from the bony cortex in the metaphyseal region of a rib and develops as a stalked mass with a cartilaginous cap. Microscopically, the amount of bony proliferation and thickness of the cartilaginous cap varies. Stippled calcification is often present within the tumor, and a rim of calcification can be present at the periphery (Fig. 49-1). The tumor begins in childhood and continues to grow until skeletal maturity is reached. The lesion may grow inward, remaining asymptomatic, or grow outward, producing a palpable mass.
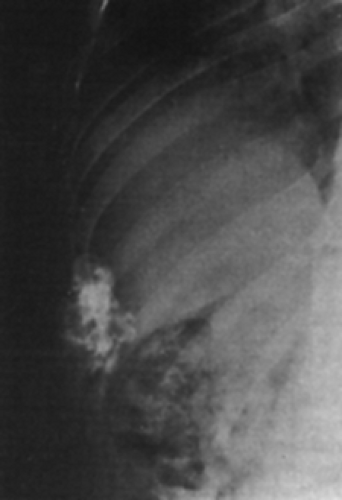 Figure 49-1. A 52-year-old man with an osteochondroma arising in the anterior right ninth rib. Note the intact cortex and stippled calcification within the tumor. (From Pairolero PC. Chest wall tumors. In Shields TW, LoCicero J III, Ponn RB, eds. General Thoracic Surgery. Philadelphia: Lippincott Williams & Wilkins, 2000:589. With permission.) |
Osteochondromas detected in children after puberty or in adults should be resected. Before puberty, resection is indicated for the onset of pain or increase in size, especially because malignant degeneration has been reported. Males are affected three times more frequently than females. Complete surgical resection is the treatment of choice. Recurrence has never been reported.
Chondroma
Chondromas represent 15% of all benign rib neoplasms, and most commonly occur in the second or third decade of life, affecting both sexes equally. They present as slowly enlarging, asymptomatic masses originating anteriorly at the costochondral junction. The radiographic appearance is that of an expansile medullary mass that causes thinning of the cortex. Clinically and radiographically, it is not possible to differentiate chondroma from chondrosarcoma. Histologically, the tumor consists of lobules of hyaline cartilage. However, the microscopic
differentiation between a chondroma and a low-grade chondrosarcoma can be difficult. Therefore, all chondromas must be managed as malignant lesions, with wide excision to prevent local recurrence.
differentiation between a chondroma and a low-grade chondrosarcoma can be difficult. Therefore, all chondromas must be managed as malignant lesions, with wide excision to prevent local recurrence.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


